
If you work in psychiatric care, whether as a provider, biller, or administrator, you already know that getting reimbursed correctly hinges on one thing: using the right Current Procedural Terminology (CPT) code. But understanding CPT codes for psychiatric evaluation goes far beyond memorizing a five-digit number.
It touches every part of your revenue cycle, from how you document a session, how you submit a claim, how auditors evaluate your records, to how your practice measures performance over time.
This guide explores all about the CPT code for psychiatric evaluation, with special focus on how each code flows into insurance claims, compliance reporting, and KPI tracking. Whether you're billing for a first-time psychiatric intake or reviewing records without ever seeing the patient, this is the reference you need.
At a Glance
- CPT codes 90791, 90792, and 90885 serve different purposes. 90791 covers non-medical psychiatric evaluations, 90792 includes medical services (e.g., prescribing), and 90885 applies to record review without patient contact.
- Documentation drives reimbursement. A complete MSE, risk assessment, DSM-5-TR diagnosis, and correct ICD-10 linkage are essential to support the CPT code billed.
- Authorization, modifiers, and POS matter. Telehealth rules (e.g., modifier 95), prior authorization, and accurate place-of-service coding directly affect claim approval.
- Common errors trigger denials. Rebilling 90791 without justification, ICD-10 mismatches, and missing documentation increase audit and revenue risk.
- Stronger coding processes protect revenue. RapidClaims helps in proactive claim checks, provider training, and compliance monitoring to reduce denials and improve financial performance.
Table of Contents
- What Is a CPT Code for Psychiatric Evaluation?
- Common CPT Codes For Psychiatric Evaluation
- How Psychiatric Evaluation CPT Codes Are Used in Billing
- How Psychiatric CPT Codes Drive Authorization & Reimbursement
- Common Mistakes To Avoid With Billing Code For Psychiatric Evaluation
- How RapidClaims Eliminates Psychiatric Billing Errors Before They Happen
- Conclusion
- FAQs
What Is a CPT Code for Psychiatric Evaluation?
A CPT (Current Procedural Terminology) code is a standardized five-digit numeric code maintained by the American Medical Association (AMA) that describes a specific medical service.
When a provider delivers psychiatric care, they assign CPT codes to each service. These codes travel with insurance claims, inform reimbursement decisions, and anchor compliance reviews.
For psychiatric evaluations specifically, the key codes fall within the 90000 series, which covers behavioral health and psychiatric services.
These are distinct from general Evaluation & Management (E/M) codes (99201–99215) or psychotherapy codes (90832–90837), though all can interact within the same billing encounter.
Read on to know more about each of them.
Common CPT Codes For Psychiatric Evaluation
The three foundational CPT codes for psychiatric evaluation are:
- 90791 – Psychiatric Diagnostic Evaluation (without medical services)
- 90792 – Psychiatric Diagnostic Evaluation with Medical Services
- 90885 – Psychiatric Evaluation of Records for Diagnostic Purposes
CPT 90791 vs. 90792 vs. 90885
| Feature | 90791 | 90792 | 90885 |
|---|---|---|---|
| Patient Contact | Yes | Yes | No |
| Medical Services Included | No | Yes | N/A |
| Can Prescribers Bill? | Yes | Yes (preferred) | Yes |
| Can Non-Prescribers Bill? | Yes | No | Yes (varies) |
| Medicare Covers? | Yes | Yes | Generally No |
| Time-Based? | No (content-based) | No (content-based) | No |
| Typical Medicare Rate | $165–$195 | $195–$230 | Not covered |
| Common Add-On | +90785 (interactive complexity) | +90785; modifier 25 | 90889 (report writing) |
| Audit Risk Level | Medium | Medium-High | Low-Medium |
| Use for Telehealth? | Yes + modifier 95 | Yes + modifier 95 | Payer-dependent |
Each has its own scope, eligible providers, billing rules, and compliance implications, all of which are covered below.
1. CPT Code 90791
CPT 90791 is the standard code for a comprehensive psychiatric diagnostic evaluation that does not include medical services. This means no prescription writing, no medication review, and no lab orders. It is the foundational intake code for most mental health providers and is almost always billed during a patient's first session with a new provider.
This code covers a full biopsychosocial assessment, including:
- Detailed psychiatric and medical history
- Mental Status Examination (MSE)
- Risk assessment (suicidality, self-harm, violence)
- Provisional DSM-5-TR diagnosis
- Initial treatment planning and goal-setting
- Family/collateral interviews when clinically indicated
Who Can Bill CPT 90791?
This code is not limited to physicians. The following qualified mental health professionals can bill 90791, subject to state regulations and payer policies:
| Provider Type | Can Bill 90791? | Notes |
|---|---|---|
| Psychiatrist (MD/DO) | Yes | May prefer 90792 if Rx is involved. |
| Psychiatric NP (PMHNP) | Yes | 90792 if prescribing. |
| Licensed Psychologist (PhD/PsyD) | Yes | Cannot prescribe; 90791 is standard. |
| Licensed Clinical Social Worker (LCSW) | Usually Yes | Verify by state and payer. |
| Licensed Professional Counselor (LPC) | Varies | Check the state scope of practice. |
| Marriage & Family Therapist (MFT) | Varies | Payer-dependent; growing acceptance. |
When to Use CPT 90791
Use CPT 90791 in these clinical scenarios:
- A new patient's initial psychiatric intake assessment
- A patient returning after a significant break in treatment (typically 6–12+ months, payer-dependent)
- A re-evaluation following a major change in diagnosis or clinical presentation
- An evaluation that includes collateral interviews but no medical services
CPT 90791 is typically a once-per-provider service. Billing it repeatedly for the same patient without documented clinical justification is a common audit trigger.
Components of a Valid CPT 90791 Evaluation
To support a 90791 claim, your documentation must reflect all required components:
1. History and Mental Status Examination: Document the chief complaint, onset and duration of symptoms, previous psychiatric diagnoses and treatments, medication history, substance use, family psychiatric history, social and developmental history, and a full Mental Status Exam (MSE). This covers appearance, behavior, mood/affect, speech, thought content and process, perceptual disturbances, cognition, and insight/judgment.
2. Risk Assessment: Evaluate and explicitly document suicidal ideation, homicidal ideation, self-harm history, and protective factors. Risk stratification (low, moderate, high) should be included. This is both a clinical necessity and a compliance checkpoint.
3. Diagnosis Using DSM-5-TR Criteria: Assign the appropriate DSM-5-TR diagnosis and pair it with the corresponding ICD-10-CM code on the claim. Vague diagnoses without diagnostic criteria documentation are a leading cause of denials and audit findings.
4. Initial Treatment Plan: Document a preliminary plan including therapeutic modality, frequency of sessions, target symptoms, short- and long-term goals, and any referrals. Insurance payers increasingly require this for authorization of ongoing services.
Always verify the patient's mental health benefits before the first session. Deductibles, out-of-pocket maximums, and prior authorization requirements vary widely, and a surprise bill after a psychiatric evaluation can damage the therapeutic relationship.
2. CPT Code 90792
CPT 90792 differs from 90791 in one critical way. It includes medical services. This means the provider performs a medical evaluation in addition to the psychiatric assessment.
This includes ordering or reviewing labs, prescribing or adjusting medication, assessing physical health factors affecting mental health, or performing a physical examination relevant to the psychiatric presentation.
This code is primarily used by psychiatrists, psychiatric nurse practitioners, and other medically licensed providers who can both diagnose and treat with medications.
Common Use Cases for CPT 90792
- A psychiatrist conducting a new patient evaluation, which includes reviewing labs and initiating medication.
- A PMHNP assessing a patient for ADHD, ordering cognitive testing, and prescribing a stimulant.
- An evaluation of an older adult where physical health factors (e.g., thyroid function) must be assessed as part of the psychiatric workup.
- Any intake evaluation where the medical history is reviewed and a prescription is written at the same visit.
If a psychologist or LCSW performs an intake, even if the patient is on medication, they use 90791, not 90792. The medical services must be provided by the billing provider at that encounter.
Best Practices for Billing CPT 90792
To avoid denials and audit risk:
- Document the specific medical service performed.
- Include the rationale for medical decision-making, not just the outcome.
- Record total time spent, including review of records, face-to-face time, and coordination.
- Use appropriate ICD-10 codes that reflect both the psychiatric diagnosis AND any medical comorbidities addressed.
- Append modifier 25 if billing an E/M code on the same day for a separate and distinct service.
3. CPT Code 90885
CPT 90885 is unique among psychiatric evaluation codes because it covers record review without direct patient contact. The provider reviews prior evaluations, treatment records, school reports, legal documents, psychological testing results, or medical records, and produces a clinical analysis that informs diagnosis or treatment planning.
This code is commonly used in forensic psychiatry, disability evaluations, second-opinion consultations, and complex cases where prior records are essential to understanding the patient's clinical picture before or between direct encounters.
Who Can Bill CPT Code 90885?
- Psychiatrists (MD/DO)
- Clinical Psychologists (PhD/PsyD)
- Psychiatric Nurse Practitioners
- Licensed Clinical Social Workers (when permitted by state law and payer policy)
- Licensed Professional Counselors and MFTs (varies significantly by state and payer)
CPT 90885 vs. Similar Codes
| Code | Service | Key Distinction |
|---|---|---|
| 90887 | Interpretation of results | Explains findings to family/responsible parties |
| 90889 | Preparation of the report | Writing a formal report based on a psychiatric evaluation |
| 96130–96133 | Psychological testing | Active administration/scoring of new tests |
| 99241–99255 | E/M Consultation | Face-to-face patient assessment required |
Medicare does not reimburse CPT 90885 as a standalone service. Many commercial payers also have restrictions. Always verify coverage before rendering service, and document medical necessity thoroughly for payers that do cover it.
Also Read: OB GYN CPT Codes: Guide to Gynecology Coding and Billing
How Psychiatric Evaluation CPT Codes Are Used in Billing
Getting the CPT code right is only the beginning. Here is how the code travels from your clinical encounter through the billing and reimbursement process.
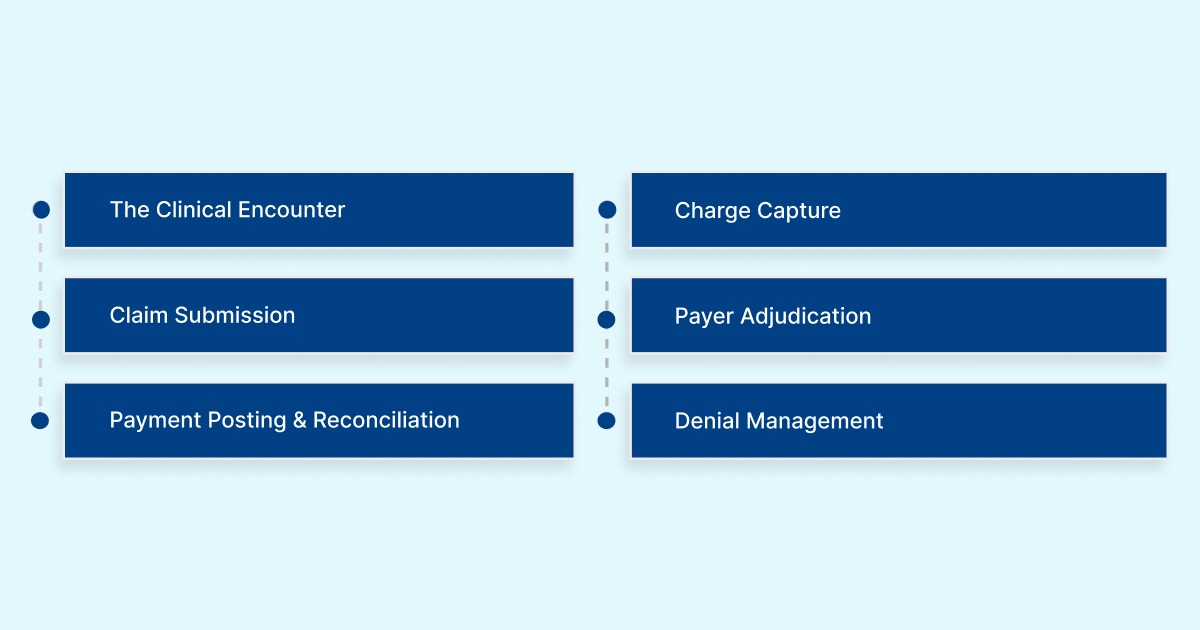
Step 1: The Clinical Encounter
The provider completes the psychiatric evaluation and documents all required components in the patient's record (EHR or paper chart). The documentation must support the CPT code billed. The completeness of the record determines both the code's defensibility and the likelihood of the claim's approval.
Step 2: Charge Capture
The biller or provider assigns the correct CPT code (90791, 90792, or 90885), links it to the corresponding ICD-10-CM diagnosis code, adds any required modifiers (e.g., 95 for telehealth, 25 for same-day E/M), and enters the Place of Service (POS) code. For outpatient office visits, this is POS 11. For telehealth from the patient's home, POS 10 (Medicare) or 02 may apply.
Step 3: Claim Submission
The claim is submitted electronically on a CMS-1500 form (or 837P electronic transaction) to the payer. Key fields that must be accurate include:
- Box 21: ICD-10 diagnosis codes (up to 12; primary diagnosis drives medical necessity)
- Box 24D: CPT code with modifiers
- Box 24B: Place of Service code
- Box 24J: Rendering provider NPI
- Box 33: Billing provider information
Step 4: Payer Adjudication
The insurance company applies several automated checks: eligibility verification, authorization requirements, frequency limitations (e.g., 90791 billed more than once per provider triggers review), LCD/NCD policy matches, and bundling edits. Mental health parity laws, under the Mental Health Parity and Addiction Equity Act (MHPAEA), require commercial insurers to cover psychiatric services at parity with medical services.
Step 5: Payment Posting and Reconciliation
Once the Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA) is received, the payment is posted to the patient account. The biller reconciles allowed amounts against expected reimbursement rates. Underpayments, denials, and adjustments are flagged for follow-up.
Step 6: Denial Management
Common denial reasons for psychiatric evaluation codes include:
- CO-4: Service not covered or authorization not obtained
- CO-11: Diagnosis inconsistent with procedure billed
- CO-97: Procedure billed as part of another procedure already adjudicated
- PR-50: Non-covered by this payer (common with 90885 under Medicare)
- CO-167: Diagnosis not covered by this payer
Each denial type has a specific resolution path, from providing additional documentation to submitting a corrected claim or formal appeal with a letter of medical necessity.
Also Read: Neurology & Neuromuscular Procedures: CPT Codes Explained
How Psychiatric CPT Codes Drive Authorization & Reimbursement
Psychiatric CPT codes are not just billing identifiers; they directly determine whether a service requires prior authorization and how much a provider is reimbursed.
Prior Authorization for Psychiatric Evaluations
Some payers require prior authorization before an initial psychiatric evaluation can be billed. Mental health parity laws limit the use of Physician Assistants for mental health when it isn't required for analogous medical services. However, many commercial plans still require authorization. Best practices include:
- Verify PA requirements at the time of scheduling, not at check-in.
- Obtain the authorization number and note it in the claim.
- Document medical necessity language aligned with the payer's clinical criteria.
- Track authorization expiration dates in your practice management system.
Telehealth Claims for Psychiatric Evaluations in 2026
The post-pandemic telehealth CPT has largely stabilized in 2026. For psychiatric evaluations via telehealth:
- 90791 and 90792 are both billable via synchronous video. Same CPT codes, same documentation requirements.
- Append modifier 95 (synchronous telehealth via interactive audio/video) for most commercial payers.
- Medicare requires a place of service code 02 (telehealth, other than the patient's home) or 10 (patient's home), depending on where the patient receives care.
- The requirement for an in-person visit within 6 months before tele-mental health has been suspended through at least late 2025 for Medicare.
- Audio-only evaluations (phone only) are permitted in specific circumstances but require a modifier CR or payer-specific codes.
Mental Health Parity and Its Impact on Claims
The MHPAEA prohibits most health plans from imposing stricter limitations on mental health benefits than on medical/surgical benefits. For billing purposes, this means:
- If a payer covers an initial E/M visit without PA, it generally cannot require PA for 90791.
- Quantitative limits (visit caps, day limits) must apply equally to mental health and medical services.
- Non-quantitative limits (prior authorization criteria, medical necessity standards) must use comparable criteria.
If your claims for 90791 or 90792 are being denied at higher rates than analogous medical codes, document the pattern and consider filing a parity complaint with your state insurance commissioner or the Department of Labor for ERISA plans.
Common Mistakes To Avoid With Billing Code For Psychiatric Evaluation
Psychiatric evaluation codes are high-value services and high-risk for denials. Small documentation or coding errors can delay authorization, reduce reimbursement, or trigger audits.
Here are the most common billing mistakes providers make with psychiatric evaluation codes and how to avoid them:
| Mistake | Risk | Prevention |
|---|---|---|
| Using 90791 when 90792 is appropriate (or vice versa) | Underpayment or compliance violation | Provider training; coder-clinician checklist |
| Billing 90791 more than once without justification | Payer audit; recoupment | Document the re-eval necessity clearly in the chart |
| Missing or vague MSE in the chart | Claim denial; documentation deficiency finding | Structured MSE templates in EHR |
| Wrong Place of Service code (telehealth vs. in-office) | Claim denial; compliance flag | POS checklist in scheduling workflow |
| Omitting modifier 95 for telehealth evaluations | Claim denial or underpayment | Billing system rules engine; payer grid |
| Billing 90885 to Medicare | Claim denial; no coverage | Payer coverage grid maintained in the billing system |
| No prior authorization for required payers | Denial: patient financial responsibility issues | PA checklist triggered at scheduling |
| ICD-10 mismatch with CPT code | CO-11 denial | Clinical documentation improvement program |
These mistakes are more common than most practices realize, and their downstream effects compound quickly. But most of these errors are preventable, not through more manual review, but through smarter systems that catch problems before they become denials.
Also Read: Top 20 Denial Codes in U.S. Medical Billing (2026 Guide)
How RapidClaims Eliminates Psychiatric Billing Errors Before They Happen
Psychiatric billing isn’t simple. You’re balancing clinical detail with strict payer rules every day. Manual processes often fall short. If your practice bills high volumes of 90791 and 90792, even a small error rate can result in significant revenue loss and increased compliance exposure.
RapidClaims is an AI-driven medical coding automation platform purpose-built to address exactly these challenges. It integrates directly into your existing EHR and billing workflows, automating coding, flagging documentation gaps before submission, and delivering real-time compliance intelligence.
We offer:
- Automated CPT & ICD-10 Coding for Psychiatric Encounters: RapidCode processes 1,000+ charts per minute with 96%+ audited accuracy, automatically assigning the correct psychiatric evaluation code (90791, 90792, or 90885) based on clinical documentation. This eliminates the human error that drives most evaluation code mismatches.
- Pre-Submission Claim Scrubbing: RapidScrub applies 119 million smart edits refreshed daily from payer bulletins, catching modifier errors, ICD-10 mismatches, missing authorizations, and bundling conflicts before a claim ever leaves your system, reducing denial rates by up to 70%.
- Documentation Gap Detection in Real Time: RapidCDI flags incomplete Mental Status Exams, missing risk assessments, and unsupported diagnoses at the point of care. This gives clinicians a chance to complete their documentation before the session closes, not after a denial arrives.
- Full Audit Trail for Every Code Assigned: Every CPT and ICD-10 code assigned by us comes with a line-level rationale and exportable audit trail, making compliance reviews, payer audits, and internal chart audits straightforward and defensible.
- Telehealth Modifier & Payer Policy Compliance: It automatically applies the correct telehealth modifiers (95, GT, GQ) and place-of-service codes based on current payer rules, keeping your psychiatric telehealth claims compliant with 2025 Medicare and commercial payer requirements without manual lookups.
- Seamless EHR Integration: RapidClaims connects with Epic, Cerner, Athena, eClinicalWorks, and other major EHR and billing platforms via SMART-on-FHIR and HL7 APIs, with implementation timelines measured in days, not months.
For psychiatric practices navigating the complexity of 90791, 90792, and 90885 billing, RapidClaims transforms coding from a reactive, error-prone process into a proactive, intelligent system.
Conclusion
The CPT code for psychiatric evaluation, 90791, 90792, and 90885, directly impact reimbursement, compliance, and audit risk. Each CPT code for psychiatric diagnostic evaluation requires precise documentation, accurate ICD-10 linkage, correct modifiers, and proper authorization.
Selecting the right initial psychiatric evaluation CPT code and supporting it with a complete MSE and risk assessment ensures your billing code for psychiatric evaluation gets approved the first time, reducing denials and revenue leakage.
RapidClaims automates this process. Our AI assigns accurate CPT and ICD-10 codes, detects documentation gaps in real time, applies telehealth modifiers correctly, and scrubs claims before submission to prevent errors.
Ready to simplify psychiatric billing and get paid faster? Book a demo today.
FAQs
1. Can the same CPT code for psychiatric diagnostic evaluation be billed by both an MD and an LCSW?
Yes, CPT 90791 can be billed by both. The key difference: MDs and PMHNPs use 90792 when medical services (like prescribing) are included. LCSWs always use 90791 regardless of complexity, as they cannot provide medical services.
2. Can you bill the billing code for psychiatric evaluation and a therapy code on the same day?
Generally, no. Most payers don't allow 90791 or 90792 to be billed alongside psychotherapy codes (90832–90837) on the same date. The evaluation is considered a standalone, comprehensive service for that visit.
3. How many times a year can the initial psychiatric evaluation CPT code be billed for the same patient?
Typically, once per provider. Re-billing 90791 is allowed only with clear clinical justification, such as a significant break in treatment or major diagnostic change. Frequency limits vary by payer; always verify before resubmitting.
4. Can the billing code for psychiatric evaluation be used for group practice supervisees billing under a supervising psychiatrist?
Yes, with conditions. Incident-to billing rules under Medicare allow this only for established patients in certain settings. For new patient psychiatric evaluations, the supervising provider must be present. State rules and payer policies vary significantly.
5. What ICD-10 codes are typically paired with the initial psychiatric evaluation CPT code 90791?
Common pairings include F32.x (Major Depressive Disorder), F41.1 (Generalized Anxiety Disorder), F31.x (Bipolar), F20.9 (Schizophrenia), and F90.x (ADHD). The ICD-10 code must reflect the documented DSM-5 diagnosis — not a symptom or rule-out.


