

Medical upcoding remains one of the most persistent compliance and revenue risks in the U.S. healthcare system. According to the Centers for Medicare & Medicaid Services (CMS), Medicare Fee-for-Service improper payments totaled approximately $28.8 billion, with documentation and coding errors consistently cited as leading contributors.
At its core, medical upcoding occurs when higher-paying codes are submitted without documentation that supports the billed level of service or complexity. Whether intentional or accidental, the outcome is the same: audits, payment recoupments, delayed reimbursements, and sustained payer scrutiny.
As chart volumes rise and coding guidelines continue to evolve, manual review processes struggle to keep up. What was once an isolated coding issue has become a systemic revenue cycle challenge.
This blog breaks down how medical upcoding occurs, how it’s detected, and how healthcare organizations are using AI-driven coding workflows to reduce risk before claims are submitted.
At a Glance
- Medical upcoding creates serious compliance and revenue risk when higher-paying codes are billed without sufficient clinical documentation, leading to audits, recoupments, and delayed reimbursements.
- Most upcoding stems from workflow and documentation gaps, not intent, driven by EHR templates, coding pressure, guideline changes, and limited real-time validation.
- Payers detect upcoding through data-driven pattern analysis, flagging code escalation, provider outliers, and severity inflation across E&M, DRG, and risk adjustment workflows.
- AI-powered coding controls prevent upcoding before submission, validating documentation in real time, reducing denials and audits, and keeping organizations audit-ready at scale.
Table of Contents
- What Is Medical Upcoding?
- Common Examples and Types of Medical Upcoding
- Medical Upcoding vs Other Coding Errors
- Why Medical Upcoding Happens in Healthcare Billing
- Where Medical Upcoding Appears in Revenue Cycle Workflows
- Common Red Flags That Indicate Medical Upcoding
- How Medical Upcoding Impacts Healthcare Organizations and Patients
- Why Medical Upcoding Is Prohibited Under U.S. Healthcare Regulations
- How Payers and Regulators Detect Medical Upcoding
- How to Prevent Medical Upcoding
- How AI Helps Prevent and Detect Medical Upcoding at Scale
- RapidClaims: AI-Driven Medical Coding and Compliance at Scale
- Final Thoughts
- FAQs
What Is Medical Upcoding?
Medical upcoding occurs when CPT, ICD-10, HCPCS, or HCC codes are reported at a higher level of service, complexity, or severity than what the clinical documentation supports. In practical terms, the claim reflects more intensive or costly care than was actually delivered.
Common examples include:
- Billing a higher-level E&M visit without sufficient medical decision-making
- Selecting a complex procedure code when a simpler service was performed
- Reporting diagnoses that inflate risk scores without clear clinical evidence
Upcoding is different from clerical miscoding or unbundling, but it often stems from the same underlying issue: documentation quality. When provider notes are incomplete or ambiguous, coders are forced to infer intent rather than rely on explicit clinical detail, increasing the risk of unsupported codes.
At the individual claim level, upcoding is difficult to spot. Payers typically identify it through comparative analysis, flagging patterns that deviate from peer benchmarks, such as sustained use of high-complexity codes or elevated diagnosis severity. These patterns often trigger audits and retrospective reviews.
Now, let’s explore how medical upcoding shows up in real-world billing scenarios.
Common Examples and Types of Medical Upcoding
While scenarios vary, the core issue is consistent: the billed code exceeds what the clinical documentation supports.
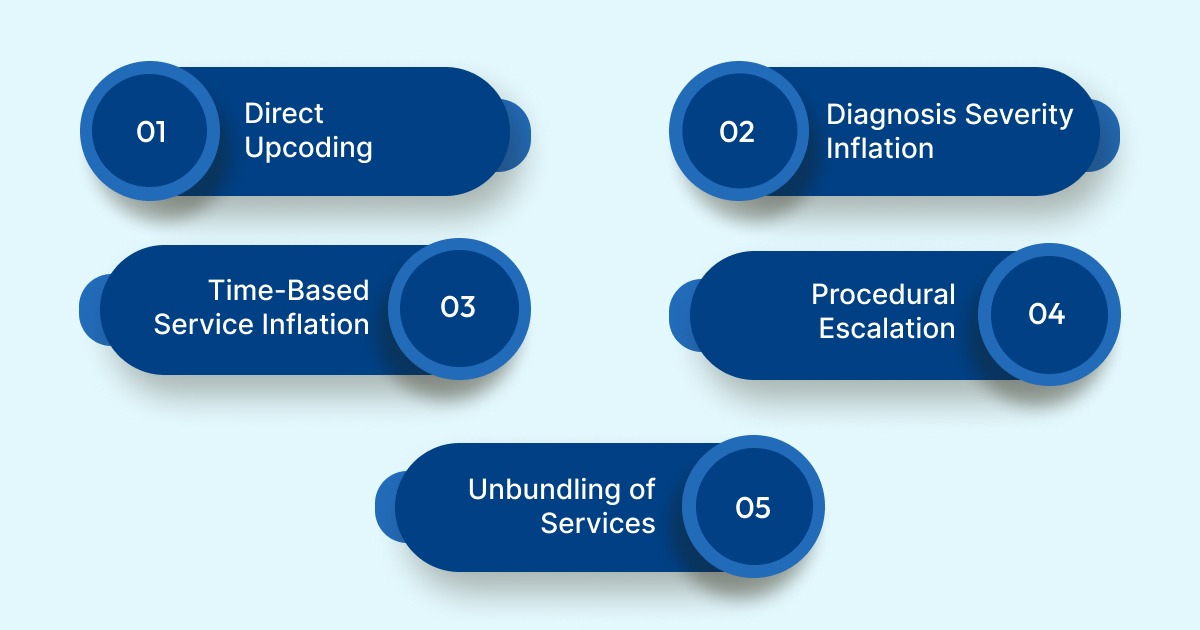
1. Direct Upcoding: Assigning higher-cost CPT codes when documentation supports a lower level of service. This is most common in E&M coding, such as billing Level 4 or 5 visits for routine encounters with limited medical decision-making.
2. Diagnosis Severity Inflation: Reporting diagnoses at a higher severity than supported by the patient record. This often appears in risk adjustment workflows, where unsupported chronic or hierarchical conditions increase reimbursement without clear clinical evidence.
3. Time-Based Service Inflation: Billing longer visit durations or extended services when documentation reflects a shorter encounter. For example, submitting claims for prolonged counseling or therapy sessions when clinical notes support only brief visits.
4. Procedure Complexity Escalation: Selecting a more complex procedure code when a standard or lower-complexity procedure was performed. This may occur when documentation lacks detail and higher-paying codes are chosen by default.
5. Unbundling of Services: Billing components of a procedure separately when they should be reported under a single bundled code. Although distinct from direct upcoding, unbundling results in similar reimbursement inflation and is reviewed under the same compliance frameworks.
Because upcoding is often confused with other billing issues, it’s important to distinguish it from related coding errors that carry different levels of risk.
Medical Upcoding vs. Other Coding Errors
Coding inaccuracies take different forms, each with distinct financial and compliance implications. Understanding these differences helps revenue cycle teams apply the right controls.
| Issue Type | Description | Primary Risk |
|---|---|---|
| Upcoding | Billing a higher-level service or complexity than what the clinical documentation supports | Audits, payment recoupments, penalties |
| Undercoding | Billing a lower-level service than what was actually provided and documented | Lost or delayed revenue |
| Unbundling | Separating services that should be billed together under a single code | Compliance violations and payer scrutiny |
| Documentation gaps | Incomplete or unclear clinical records that do not fully support coded services | Denials and adverse audit findings |
Among these, upcoding carries the highest regulatory risk because it directly inflates reimbursement. While it can be intentional, it more often results from documentation gaps, guideline misinterpretation, or workflow constraints. Without timely validation, these issues can persist and surface later through payer reviews or audits.
Also Read: Unbundling and Upcoding Key Differences Explained
Why Medical Upcoding Happens in Healthcare Billing
Medical upcoding rarely results from a single mistake. It typically emerges when financial incentives, documentation challenges, operational pressure, and regulatory complexity converge within revenue cycle workflows.

Here are the key drivers of medical upcoding:
1) Payment and Incentive Structures
Diagnosis-based reimbursement models tie payment directly to coded severity. In programs such as Medicare Advantage risk adjustment, even small changes in diagnosis selection or acuity can materially affect reimbursement. Without effective validation guardrails, this creates pressure to capture higher-severity codes, increasing the risk of unsupported coding.
2) Documentation Gaps and Complexity
Clinical documentation often lacks the specificity required to support higher-level codes. Missing details related to acuity, laterality, chronicity, or clinical rationale force coders to interpret intent rather than rely on explicit evidence. EHR templates, copy-forward behaviors, and ambiguous language further increase the likelihood of unsupported code selection.
3) Operational Strain on Coding Teams
Coding teams face rising chart volumes, tighter turnaround expectations, and limited time to query providers for clarification. At the same time, they must keep pace with frequent updates to CPT, ICD-10, and HCC guidelines. In this environment, manual review processes struggle to consistently identify inconsistencies across large claim populations.
4) Regulatory and Guideline Volatility
Ongoing changes such as HCC v24 to v28 transitions, E&M guideline updates, and payer-specific edits introduce variability that is difficult to manage at scale. Without automated, rules-aware validation, organizations may unintentionally apply outdated or misaligned coding logic.
5) Process Limitations and Human Factors
Manual review processes do not scale efficiently, allowing unsupported codes to reach submission when no real-time checkpoint exists. In limited cases, higher-level codes may also be deliberately selected to increase reimbursement, creating direct compliance exposure.
These underlying causes don’t exist in isolation. They tend to surface repeatedly within specific revenue cycle workflows where interpretation and pressure intersect.
Where Medical Upcoding Appears in Revenue Cycle Workflows
Medical upcoding most often develops through breakdowns in documentation and coding workflows, not from a single incorrect decision. High claim volumes, tight submission timelines, and limited review capacity increase the likelihood that higher-level codes are selected when documentation is incomplete or unclear.
Risk rises when provider notes lack specificity, documentation standards differ across departments, or coders cannot obtain timely clarification. In these conditions, manual reviews rely on individual judgment rather than consistent validation, allowing unsupported coding patterns to persist.
Upcoding appears most frequently in workflows that depend on interpretation rather than discrete clinical actions, including:
- Outpatient E&M leveling
- Inpatient DRG assignments influenced by secondary diagnoses
- Medicare Advantage risk adjustment coding
- Procedure coding driven by templated EHR notes
When identified, these patterns trigger audits, retrospective reviews, and payment recoupments. The resulting rework slows cash flow, increases administrative burden, and diverts revenue cycle teams from processing claims to responding to audits.
Without standardized documentation, clear coding guidance, and real-time validation, unsupported coding can become systemic before it is detected.
Because these workflows are high-risk, they also generate early warning signals that compliance and revenue integrity teams can monitor proactively.
Common Red Flags That Indicate Medical Upcoding
Medical upcoding is often revealed when submitted CPT or diagnosis codes do not align with the documented level of service. Identifying these warning signs early allows revenue integrity and compliance teams to intervene before payer reviews or audits occur.
Common red flags include:
- Inconsistent Billing Patterns: Claims reflect unusually high charges or services that are not clearly supported by encounter documentation.
- Frequent Code Escalation: CPT or diagnosis codes trend toward higher complexity levels without corresponding changes in clinical detail or patient acuity.
- Repeated Charges for Similar Services: Multiple claims for comparable procedures within a short timeframe may indicate inflated or redundant coding.
- Services Lacking Medical Necessity: Billed procedures are not clearly justified based on clinical notes, care plans, or treatment rationale.
- Fragmented Billing For Bundled Services: Procedures that are typically billed together appear as separate line items, increasing total reimbursement without additional care delivered.
These patterns are often identified internally through coding reviews, analytics, or staff oversight rather than external audits. When these red flags go unnoticed or unaddressed, the consequences extend well beyond individual claims.
How Medical Upcoding Impacts Healthcare Organizations and Patients
Medical upcoding is often viewed as intentional misconduct, but in practice it more commonly results from operational gaps. Complex coding guidelines, inconsistent documentation, and high-volume billing environments increase the likelihood of unsupported coding even in well-intentioned organizations.
Impact on Healthcare Organizations
When irregular coding patterns are identified, the consequences extend beyond individual claims and affect the entire revenue cycle.
- Retrospective Audits and Reviews: Payers may initiate audits that require extensive chart review and documentation defense.
- Delayed Reimbursements and Recoupments: Payment takebacks and reimbursement delays disrupt cash flow and increase A/R days.
- Higher Denial Rates: Once flagged, future claims often face closer scrutiny, leading to more denials.
- Increased Compliance and Legal Exposure: Repeated findings can escalate into sustained payer monitoring and potential exposure under the False Claims Act.
- Reputational and Contracting Risk: Ongoing issues erode payer trust, weaken contracting leverage, and create long-term revenue instability.
Impact on Patients
While providers carry regulatory accountability, patients also experience downstream effects.
- Higher Out-of-Pocket Costs: Unsupported coding can raise copayments, coinsurance, or deductibles.
- Billing Confusion and Disputes: Patients may receive charges that do not align with their understanding of the care provided.
- Downstream Clinical Risk: Inaccurate documentation can influence future treatment decisions, affecting continuity of care.
- Erosion of Patient Trust: Repeated billing discrepancies can weaken confidence in providers and care teams.
These consequences persist because upcoding rarely stems from a single failure. Vague documentation, EHR templates that imply higher complexity, productivity pressure on coding teams, frequent guideline changes, and limited real-time validation allow unsupported coding to scale across encounters before it is detected.
As a result, many organizations now approach upcoding as a systemic revenue cycle issue, requiring proactive validation, consistent documentation standards, and ongoing monitoring to manage risk effectively.
Given these consequences, it’s not surprising that medical upcoding is treated as a serious regulatory concern.
Why Medical Upcoding Is Prohibited Under U.S. Healthcare Regulations
Medical upcoding is prohibited because it results in reimbursement that is not supported by clinical documentation, leading to improper use of public healthcare funds and undermining program integrity. When claims submitted to Medicare, Medicaid, or other government-funded programs reflect higher levels of service or complexity than what was actually provided, they create financial waste and compliance exposure.
Submitting unsupported claims may violate federal statutes such as the False Claims Act, which governs the accuracy of billing to government healthcare programs.
Enforcement is not limited to intentional misconduct. Weak documentation standards, insufficient oversight, or ineffective controls can also trigger payer scrutiny and regulatory action.
Organizations that permit unsupported coding may face payment recoupments, civil penalties, increased audit frequency, and ongoing monitoring. In severe cases, consequences can include exclusion from federal programs or criminal enforcement. The determining factor is not intent alone, but whether billed services can be substantiated through clear, audit-ready documentation.
To enforce these regulations, payers and government agencies rely on increasingly sophisticated methods to identify unsupported coding patterns.
How Payers and Regulators Detect Medical Upcoding
Payers and regulators rely on a mix of analytics, benchmarking, and targeted reviews to identify medical upcoding. Detection is increasingly automated, allowing unsupported coding patterns to be surfaced at scale rather than through isolated claim reviews.
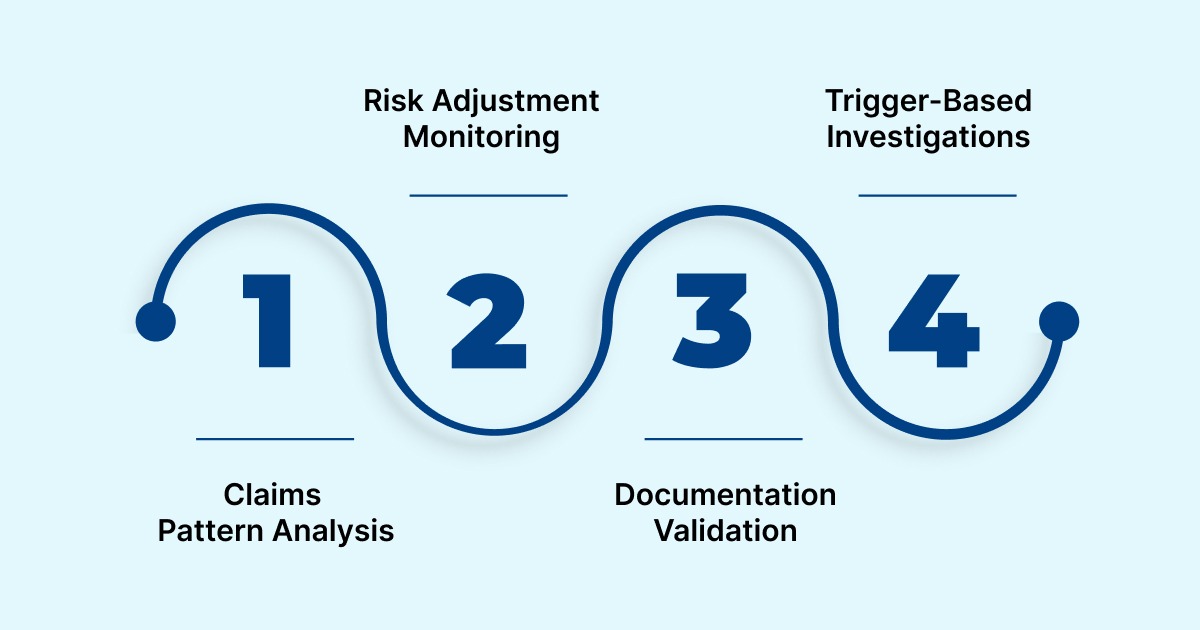
- Claims Pattern Analysis: Claims data is continuously monitored for indicators such as sudden increases in high-complexity codes, provider behavior that deviates from peer benchmarks, or inconsistent coding across similar patient populations and time periods.
- Risk Adjustment Monitoring: In Medicare Advantage programs, regulators track changes in RAF scores over time. Rapid score growth without corresponding clinical documentation often triggers focused audits and retrospective reviews.
- Documentation Validation: When patterns are flagged, claims are compared directly against medical records to confirm that billed codes are supported by clinical evidence. Gaps between documentation and coding frequently lead to recoupments.
- Trigger-Based Investigations: Prior audit findings, whistleblower reports, and unusual payment trends within specific specialties or service lines can prompt targeted investigations.
Once identified, organizations may face multi-year retrospective reviews, increasing financial exposure and ongoing regulatory oversight. Detection alone, however, is not enough. Reducing risk requires controls that prevent unsupported coding before claims are submitted.
Strategies to Prevent Medical Upcoding
Preventing medical upcoding requires controls embedded directly into daily revenue cycle workflows. One-time training and retrospective audits are not sufficient in high-volume, fast-moving billing environments.
a) Documentation Governance: Consistent documentation standards are the foundation of prevention. Standardized clinical templates, clear expectations for required specificity on high-risk codes, and ongoing provider education aligned with payer requirements reduce ambiguity at the source.
b) Coding Quality Assurance: Pre-submission validation helps identify unsupported codes before claims are filed. Targeted reviews of high-risk services and structured feedback between coders and clinicians reduce repeat issues and improve accuracy.
c) Workflow Ownership and Escalation: Clear escalation paths ensure documentation gaps are resolved consistently. Defined ownership across coding, compliance, and billing teams prevents issues from being deferred under time pressure.
d) Limits of Manual Controls: As claim volumes increase, manual reviews and sample-based audits struggle to scale. Retrospective checks often surface upcoding only after payer intervention, when financial and compliance impact is already realized.
Effective prevention depends on real-time validation that operates before claims are submitted, not after.
How AI Helps Prevent and Detect Medical Upcoding at Scale
AI reduces medical upcoding by embedding validation directly into coding workflows, shifting control from retrospective audits to real-time prevention.
- Real-Time Documentation Validation: AI analyzes structured data such as CPT, ICD-10, and modifiers alongside clinical notes to identify cases where billed codes are not supported by documentation. Pattern analysis also highlights provider- or service-level deviations from historical and peer benchmarks.
- Pre-Submission Risk Prevention: Issues are flagged while the chart is still open. Missing documentation, unsupported diagnoses, or inflated code levels can be corrected before claims are submitted, reducing downstream audits and rework.
- Audit-Ready Transparency: Each flagged or suggested code includes clear supporting evidence, the rationale for the recommendation, and a record of who approved the final decision. This simplifies audit response and payer reviews.
- Human-Controlled Workflows: AI supports coders and auditors by surfacing risk, not replacing judgment. Final coding decisions remain with human reviewers.
- Integrated Deployment: AI validation connects directly to EHR and claims systems, allowing organizations to apply consistent controls without disrupting existing workflows.
Platforms like RapidClaims apply this approach within routine coding operations, allowing organizations to prevent upcoding proactively rather than responding after payer intervention.
RapidClaims: AI-Driven Medical Coding and Compliance at Scale
RapidClaims is an AI-powered medical coding and revenue cycle platform designed to improve coding accuracy, reduce compliance risk, and scale operations without adding manual workload. It integrates with existing EHR and billing systems to embed validation into everyday workflows.
Core Products
- RapidCode: Autonomous coding for procedures, diagnoses, E&M, and risk adjustment. Analyzes documentation in real time to ensure codes are fully supported.
- RapidScrub: Pre-submission claim validation that identifies coding and compliance issues before filing, improving clean claim rates and reducing denials.
- RapidCDI: Clinical documentation improvement and risk adjustment support that surfaces documentation gaps and missing specificity.
Key Capabilities
- Real-time validation of codes against clinical documentation
- Detection of unsupported or inflated coding
- Audit-ready evidence trails for compliance reviews
- Support for evolving CPT, ICD-10, HCC, and payer-specific rules
- Seamless integration with existing revenue cycle workflows
By embedding AI directly into coding and review processes, RapidClaims helps organizations shift from retrospective audits to proactive prevention, reducing upcoding risk while maintaining speed, accuracy, and audit readiness.
Final Thoughts
Medical upcoding creates real financial, regulatory, and operational risk for healthcare organizations. In today’s high-volume, high-complexity billing environments, traditional controls alone are no longer enough to manage that exposure.
AI-powered platforms allow revenue cycle and compliance teams to identify risk earlier, validate documentation in real time, and maintain audit-ready records without slowing coding operations. By shifting prevention upstream, organizations can reduce recoupments, limit audits, and protect long-term revenue integrity.
Learn how RapidClaims helps healthcare organizations reduce medical upcoding risk while improving coding accuracy and compliance. Explore RapidClaims or request a demo now!
FAQs
1. Is medical upcoding always considered fraud?
No. Intent matters. However, even unintentional upcoding can still lead to payment recoupments, penalties, and increased scrutiny once identified during audits.
2. Which services carry the highest upcoding risk?
Evaluation and Management visits, high-complexity procedures, and risk-adjusted diagnoses are most frequently audited.
3. How can revenue cycle teams identify early signs of upcoding?
Common indicators include sudden increases in high-complexity codes, provider behavior that deviates from peer benchmarks, and unexplained growth in RAF scores.
4. Does upcoding risk vary by payer or region?
Yes. Payer policies, audit thresholds, and enforcement patterns differ by program and geography, making configurable rules and updates essential.
5. How does AI help without disrupting clinicians?
AI evaluates documentation already entered in the EHR and flags gaps or inconsistencies during coding, prompting clarification rather than adding steps to clinical workflows.
6. How does AI avoid false positives?
Effective systems combine clinical context, historical patterns, and configurable thresholds, with final decisions remaining under human review.

.jpg)
.jpg)