

Can downcoding increase reimbursements? No, it's not. Downcoding cuts your reimbursements, not increases them.
The myth exists because some providers believe using lower codes reduces denials, speeds up payment, and ultimately nets more money. That logic breaks down fast once you look at the numbers.
This blog covers what downcoding actually is, how it differs from upcoding and undercoding, why it happens, which specialties take the hardest hit, and, most importantly, how to stop it.
At a Glance
- Downcoding never increases reimbursements. A 99215 paid as 99213 can cost $60–$80 per visit, translating to $18K–$24K in monthly losses for a 300-claim E/M practice.
- It’s triggered by incomplete documentation, weak medical necessity linkage, payer AI adjudication, and outdated CPT/E/M knowledge.
- The impact goes beyond single claims: suppressed RAF/HCC capture, distorted A/R metrics, higher audit risk, and permanent revenue leakage because most downcoded claims are never appealed.
- Prevention requires system-level controls: clear MDM/time documentation, rolling internal audits, updated coding training, and payer-specific edit monitoring before claims go out.
- RapidClaims closes the gap. RapidCode ensures accurate CPT/E/M selection, RapidCDI flags documentation gaps before sign-off, RapidScrub applies 119M+ smart edits pre-submission, and RapidRecovery automates appeals, helping practices reduce denials, increase clean claim rates, and recover lost revenue within 30 days.
Table of Contents
- What Is Downcoding in Medical Billing?
- Upcoding vs. Downcoding: What’s the Difference?
- Can Downcoding Increase Reimbursements?
- 5 Common Causes of Downcoding
- 7 Financial Impact of Downcoding on Medical Billing and Reimbursements
- Which Specialties Are Most Affected by Downcoding?
- How to Prevent Downcoding
- How RapidClaims Helps You Stop Downcoding Before It Starts
- Conclusion
- FAQs
What Is Downcoding in Medical Billing?
Downcoding happens when a claim is reimbursed at a lower service level than what was billed. You submit a claim for a high-complexity visit, CPT 99215, and the payer pays it as a moderate visit, CPT 99213. The service happened. The documentation exists. But you get paid less.
This gap costs providers real money on every single encounter.
Payers typically downcode when their system determines the documentation does not fully support the billed level. Sometimes it's a human reviewer. Increasingly, it's an automated algorithm that flags the claim within milliseconds.
Downcoding is often confused with undercoding. They are related, but they work in opposite directions and carry very different risks.
Downcoding vs. Undercoding: Are They the Same?
Downcoding and undercoding are not exactly the same. They produce the same financial outcome, lower reimbursement, but they come from different sides of the claim.
- Downcoding is payer-initiated. After you submit a claim, the payer’s adjudication system reviews the documentation and reimburses at a lower service level than what you billed.
- Undercoding is provider-initiated. Your coding team voluntarily bills a lower code, often to avoid denials or because the documentation looks incomplete.
Both result in lost revenue. But downcoding is done to you, while undercoding is something your practice does to itself. You can’t always stop a payer from downcoding a claim, but you can stop your team from undercoding before the claim ever goes out.
Now, let’s find out the difference between upcoding and downcoding.
Upcoding vs. Downcoding: What’s the Difference?
Both upcoding and downcoding create compliance exposure under NCCI (National Correct Coding Initiative) guidelines. Upcoding is a fraud risk. It can trigger audits, financial penalties, and legal action under the False Claims Act. Downcoding is a revenue risk. Providers lose legitimate reimbursement they earned but couldn't fully substantiate.
Here's how they compare:
| Aspect | Upcoding | Downcoding |
|---|---|---|
| Definition | Billing a higher code than performed | Reimbursed at a lower code than billed |
| Who Initiates | Provider | Payer (or provider) |
| Financial Effect | Inflated reimbursement | Reduced reimbursement |
| Compliance Risk | Fraud — False Claims Act violation | Revenue loss; still violates NCCI if intentional |
| Common Trigger | Deliberate or negligent billing | Incomplete documentation or payer AI audit |
A common misconception is that downcoding is the “safe” alternative to upcoding. It is not. Intentional underbilling is still a compliance violation, and systematic patterns of it show up in payer data. The only compliant path is accurate coding, supported by complete documentation, applied consistently across your billing team.
So why do some providers still believe downcoding can help their revenue?
Can Downcoding Increase Reimbursements?
No, downcoding never increases reimbursements. Here's why the myth persists and why it's wrong.
The Myth
- Lower codes = fewer documentation requirements = fewer denials = faster payment.
- Faster payment = better cash flow = effectively "more" revenue.
The Reality
Even if a downcoded claim pays faster, you are collecting less per encounter. At scale, that difference is significant.
- A 99215 reimburses approximately $160–$175 under Medicare rates.
- A 99213 reimburses approximately $90–$110.
- That's a $60–$80 loss per encounter.
- For a practice submitting 300 E/M claims per month, that's $18,000–$24,000 in monthly revenue left on the table.
No payment speed makes up for that. The only way to increase reimbursements is to code accurately, document completely, and submit clean claims at the correct level.
Also Read: Medical Coding Compliance: Reducing Errors and Denials
Now that we have established what downcoding costs you, the next question is, why does it happen in the first place?
5 Common Causes of Downcoding
Most downcoded claims trace back to one of five root causes. Understanding them helps you close the gaps before claims go out the door.
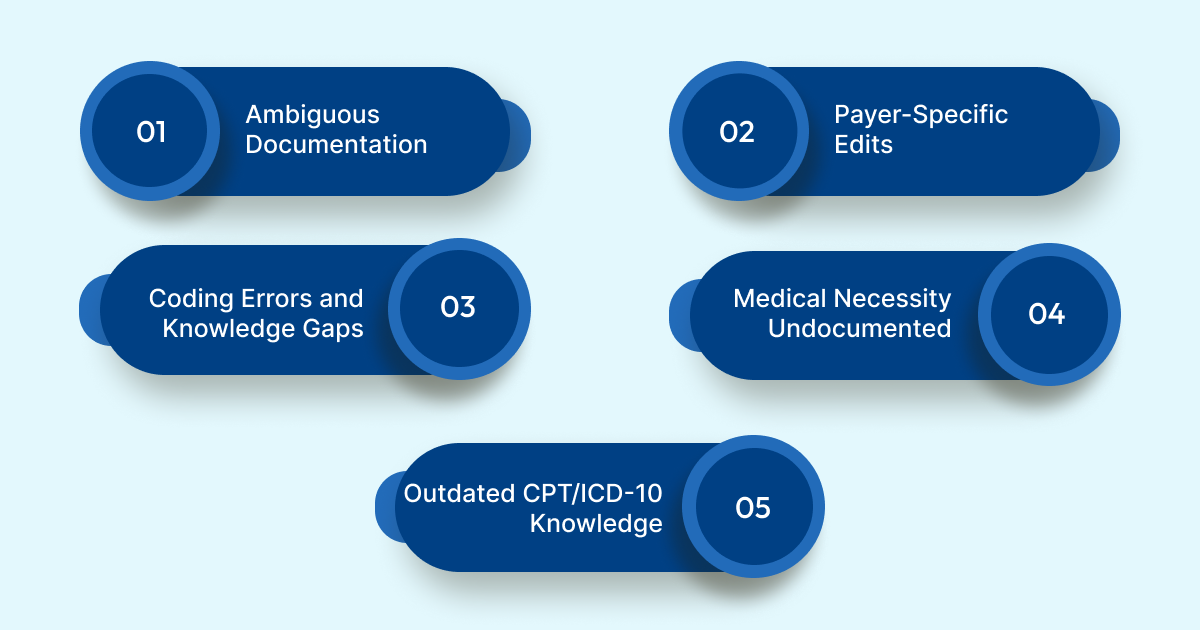
1. Incomplete or Ambiguous Documentation
This is the most cited cause across the industry. When clinical notes don't clearly state the time spent, the complexity of medical decision-making (MDM), or the problems addressed, payers default to a lower code. Specific gaps include:
- No explicit total time documented for time-based E/M billing.
- Vague MDM rationale. For example, writing 'labs reviewed' without linking findings to clinical decisions.
- Missing or incomplete risk assessment.
2. Payer-Specific Edits and Algorithmic Adjudication
Commercial payers now use proprietary AI-based adjudication systems that reassess code levels based on internal benchmarks, not just your documentation. These systems are not publicly disclosed, which makes them hard to anticipate.
For example, Cigna's Evaluation and Management Coding Accuracy policy allows automatic downcoding when its algorithm determines documentation does not support the billed level, often without any human review of the actual chart.
3. Coding Errors and Knowledge Gaps
When coding teams misapply current CPT or ICD-10 guidelines, or aren't up to date with specialty-specific rules, they select lower-level codes than the documentation supports. This is especially common during guideline transitions, like the 2021 E/M updates.
4. Lack of Medical Necessity Documentation
Medical necessity is the backbone of claim justification. When notes don't connect the patient's condition to the level of service rendered, payers have grounds to downcode. This is about diagnosis codes as well as clinical narrative.
5. Outdated Knowledge of CPT/ICD-10 Guidelines
Guidelines change. V28 HCC model updates, 2021 E/M restructuring, and annual CPT additions catch many coding teams off guard. Outdated knowledge directly translates to under-coded or incorrectly coded claims, both of which lead to downcoding or denials.
Now, let's understand how it affects medical billing and reimbursements.
7 Financial Impact of Downcoding on Medical Billing and Reimbursements
Downcoding doesn't just affect one claim. It creates a pattern of revenue leakage that's hard to detect and even harder to recover from after the fact. Here's what it looks like financially:
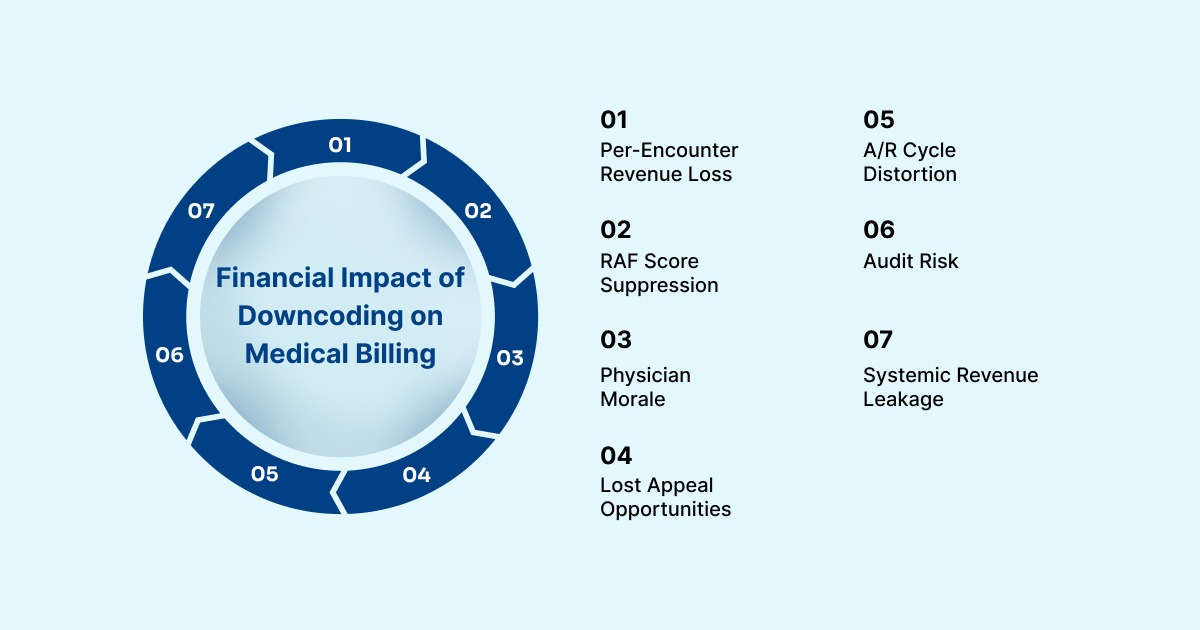
1. Per-Encounter Revenue Loss: A single downcoded E/M visit can cost $60–$80. Multiply that by hundreds of claims per month, and the losses reach into the tens of thousands.
2. A/R Cycle Distortion: Downcoded claims often close faster in your A/R, which masks the revenue gap. Your denial rate looks clean, but net reimbursement per claim is lower.
3. RAF Score Suppression: For Medicare Advantage and ACO contracts, chronic downcoding suppresses HCC capture, lowering your Risk Adjustment Factor (RAF) score and reducing capitation payments.
4. Audit Risk: Consistent patterns of high-level billing followed by payer downcoding can trigger pre-payment reviews or post-payment audits, adding administrative burden.
5. Physician Morale: When physicians see their clinical work repeatedly valued below what they documented, it creates frustration and drives documentation fatigue, which then worsens the problem.
6. Systemic Revenue Leakage: Studies estimate that most of the revenue leakage in healthcare practices is tied to coding inaccuracies, including downcoding.
7. Lost Appeal Opportunities: Most downcoded claims are never appealed. Providers accept the lower payment, so the revenue is gone permanently.
Downcoding is quiet by design. It doesn't trigger a denial. It doesn't generate a worklist item. It just pays less.
Downcoding hits every specialty. But some practices are targeted more aggressively than others. Here’s where the exposure is highest.
Which Specialties Are Most Affected by Downcoding?
Downcoding impacts nearly every specialty, but some are hit harder based on the complexity of their services and the documentation standards payers apply.
Emergency Medicine
Emergency physicians are among the most affected. Payers frequently downcode E/M codes for ED visits, arguing that documentation doesn't meet the threshold for high-acuity billing. This directly violates the Prudent Layperson Standard, which requires payer reimbursement based on a patient's presenting symptoms — not the final diagnosis. Despite this legal protection, automated adjudication systems continue to downcode ED claims.
Primary Care — E/M Codes 99213–99215
After the 2021 E/M guideline changes, legitimate use of Level 4 and Level 5 codes increased across primary care. Payers responded by flagging providers whose coding profiles sat above peer averages, even when the higher-level codes were fully justified. The result: widespread downcoding of 99214 and 99215 claims.
Behavioral Health
Behavioral health providers face downcoding related to session length and therapeutic service documentation. Payers require precise documentation of session time and modality. When notes are vague or templated, claims get downcoded, often silently.
Surgery, Cardiology, and Orthopedics
High-value procedure codes in surgical and specialty care are frequent targets. Payers apply bundling rules and NCCI edits that can reduce the payable components of a claim. Without specific documentation of distinct procedures and clear medical necessity, multiple codes get collapsed into a single lower reimbursement.
Across all specialties, the pattern is the same: inadequate documentation gives payers the justification to pay less. The next step is to build a system that stops it before claims go out.
How to Prevent Downcoding
Prevention starts before the claim leaves your system. Here's where to focus your efforts.
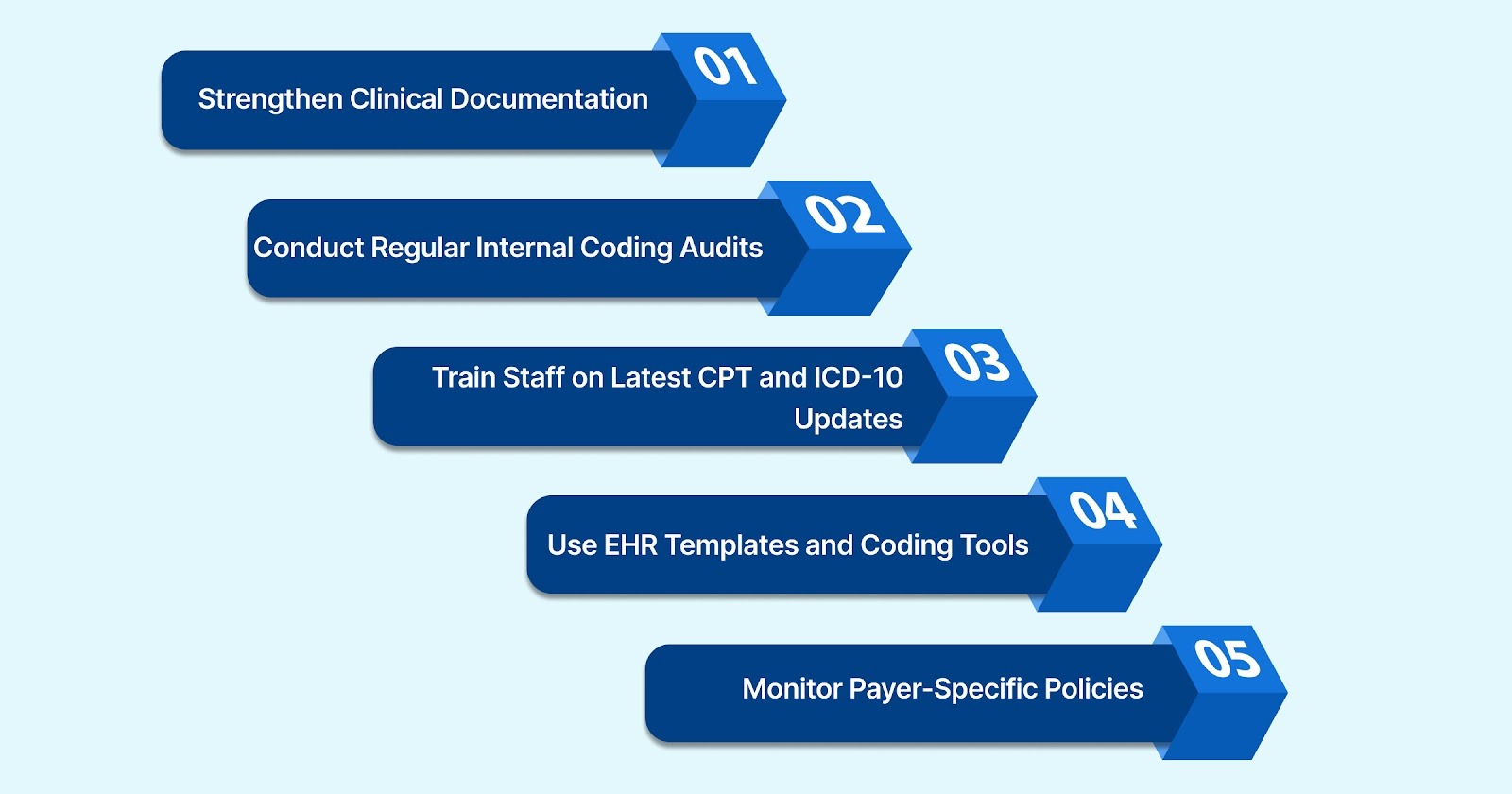
1. Strengthen Clinical Documentation
Every note should explicitly state total time, MDM rationale, the number of problems addressed, the data reviewed, and how it influenced clinical decisions. Ambiguity in the chart is ammunition for payer downcoding. Specificity is your defense.
2. Conduct Regular Internal Coding Audits
Run audits on a rolling basis, not just annually. Focus on your most-billed CPT codes and compare what's documented against what's billed. Flag patterns before payers do.
3. Train Staff on Latest CPT and ICD-10 Updates
Guidelines change every year. Your coding team needs regular training on E/M updates, specialty-specific rules, and HCC V28 transitions. A gap in knowledge at the coder level becomes a gap in reimbursement at the payer level.
4. Use EHR Templates and Coding Tools
Structured EHR templates reduce documentation gaps by prompting physicians to complete required fields, time, MDM components, and diagnosis linkage. Pair these with AI-assisted coding tools like RapidCode that flag missing elements before claim submission.
5. Monitor Payer-Specific Policies
Commercial payers update their adjudication rules frequently. Cigna, Aetna, and UnitedHealthcare all have proprietary editing policies that affect how your claims are processed. Subscribe to payer bulletins. Track policy changes. Adjust documentation standards accordingly.
But these prevention strategies work best when they are built into your workflow. That’s where RapidClaims comes in.

How RapidClaims Helps You Stop Downcoding Before It Starts
Manual coding workflows, documentation gaps, and opaque payer rules create the exact conditions that lead to downcoding. Coding teams work at capacity. Physicians don't have time to fix notes after the fact. And payer AI systems are getting faster and more aggressive, identifying and adjusting claims before a human ever reviews them.
RapidClaims is an AI-powered Revenue Cycle Intelligence platform built to close these gaps at the source. Here's how each module addresses the root causes of downcoding directly:
- RapidCode: Autonomous ICD-10, CPT, and E/M coding across 36+ specialties with 96%+ audited accuracy. It includes a real-time E/M calculator with MDM-aware scoring. So codes are selected at the right level before the claim goes out. Coder productivity lifts 170%, which means fewer errors from fatigue and overload.
- RapidCDI: Point-of-care AI prompts surface HCC gaps and RAF delta before a physician signs off on the note. Physicians see exactly which documentation elements are missing and what revenue impact that creates, in real time. This directly addresses the documentation gaps that trigger payer downcoding.
- RapidScrub: 119 million smart edits, machine-learned and refreshed daily from payer bulletins. This helps you catch claim-level errors before submission. It includes a Denial Probability Score that flags high-risk claims for human review, so your team focuses attention where it matters most.
- RapidRecovery: When downcoding does happen, the Automated Appeals Engine drafts payer-specific appeal letters, e-submits them, and tracks responses. Help you reducing appeal cycle time by 50%. Every recovered claim feeds back into RapidScrub's learning loop, improving future prevention.
Providers using RapidClaims have seen a 40% reduction in denials, a 98% clean claim rate, and a 24% HCC capture uplift, with results visible within 30 days.
Conclusion
Downcoding is a silent revenue drain. It doesn't create denials. It doesn't generate alerts. It just pays less, claim after claim, until the pattern compounds into millions in lost reimbursement annually.
The answer is not to code conservatively. It's to document completely, audit consistently, and use technology that catches the gap before the payer does.
RapidClaims helps providers do exactly that. From AI-powered coding and real-time documentation prompts to smart claim scrubbing and automated appeals. If your practice is experiencing unexplained reimbursement drops or high E/M code downcoding rates, the time to act is before the next claim goes out.
Book a demo with RapidClaims and see your projected revenue impact in 30 days.
FAQs
Q. Is downcoding illegal?
It depends on who initiates it and why. Payer-initiated downcoding based on clinical review is generally within their contractual rights. However, when payers downcode claims without reviewing actual records — or in violation of contracts or the Prudent Layperson Standard — it may be subject to legal challenge. Provider-initiated downcoding that's intentional and systematic can also raise compliance flags under NCCI guidelines. Always document accurately and code to the level the record supports.
Q. Can downcoding increase reimbursements? True or False.
False. Downcoding reduces reimbursements by assigning a lower code than the performed service justifies. There is no scenario in which downcoding results in higher payment.
Q. What's the difference between downcoding and undercoding?
Downcoding is payer-initiated — the insurer reduces the code level at adjudication. Undercoding is provider-initiated — your team voluntarily selects a lower code, usually out of caution or due to incomplete documentation. Both result in lower reimbursement. Neither is the right approach.
Q. How do I know if my claims are being downcoded?
Look for patterns in your remittance data: claims paid at a lower code than billed, reimbursement amounts that don't match your contracted rates, or a steady decline in average payment per E/M encounter. Payment variance reports and denial analytics tools can surface these patterns quickly. If you're seeing consistent gaps between billed and paid codes without denials, downcoding is likely the cause.
Q. Can I appeal a payer's downcoding decision?
Yes. You have the right to appeal downcoded claims. A successful appeal requires clinical documentation that clearly supports the billed code level. A written rationale referencing applicable CPT guidelines. And if the payer used an AI adjudication system, a request for human review. AMA provides sample appeal letter templates specifically for E/M downcoding disputes.

.jpg)
.jpg)