2026 Telehealth Updates: Key E/M Code Changes & Medicare Policies
Telehealth remains one of healthcare’s most valuable innovations, but in 2026, the reimbursement and coding landscape is shifting again.
Following the expiration of pandemic-era waivers and the release of the CMS 2025 Physician Fee Schedule (PFS), providers must adapt to new CPT® codes, tighter Medicare recognition criteria, and partial rollbacks of temporary flexibilities.
For coding and revenue cycle teams, this isn’t just a compliance update; it’s an operational one.
Each telehealth service must now align with new documentation, E/M categorization, and payer acceptance rules, or risk higher denial rates and administrative delays.
Key Takeaways
- Most 2025 telehealth flexibilities have ended: Temporary COVID-era waivers expired on December 31, 2024, marking a return to pre-pandemic coverage rules.
- Medicare recognized only one new telehealth E/M code: CPT® 98016 replaced HCPCS G2012, while 16 other new telehealth codes were not reimbursed.
- Behavioral and mental health telehealth coverage became permanent, ensuring continued patient access regardless of geographic restrictions.
- Geographic and location limits were reinstated: Only patients in rural or Health Professional Shortage Areas remain eligible for most Medicare telehealth services.
- AI-driven coding helps maintain compliance: Platforms like RapidClaims automatically update code sets and payer rules to prevent denials.
Table of Contents:
- What Changed for Telehealth Coding in 2026?
- Key 2026 Telehealth Policy and Coding Changes
- New E/M Codes for Telehealth in 2026
- How These Updates Affect Coding Operations and Compliance
- Legislative Outlook: Will Congress Intervene?
- Preparing for 2026: Key Steps for Providers and Coding Teams
- Final Thoughts
- FAQs
What Changed for Telehealth Coding in 2026?
During the COVID-19 public health emergency (PHE), Medicare expanded telehealth coverage, allowing services from nearly any location, including a patient’s home, and flexible coding for audio and video encounters.
Those flexibilities began to phase out after May 2023 and were temporarily extended under the Consolidated Appropriations Act of 2023.
The 2025 CMS Physician Fee Schedule, finalized on November 1, 2024, outlined which policies would remain, which would expire, and which would be replaced. These updates took effect on January 1, 2025, reshaping how telehealth services were coded and reimbursed.
In summary:
- Most temporary waivers expired on December 31, 2024.
- Behavioral health coverage became permanent under Medicare.
- New E/M CPT® codes were introduced for 2025.
- Medicare did not recognize most new telehealth codes.
- Direct supervision via telehealth continued through 2025.
- Geographic restrictions returned for most Medicare telehealth services.
Also Read: 2025 Guide to ICD-10 Code for Telehealth Visit Accuracy
Key 2026 Telehealth Policy and Coding Changes
This section summarizes the most important updates announced in the 2026 CMS Final Rule and the related AMA CPT® changes.
Also Read: Telehealth Place of Service Code for Medical Coders
New E/M Codes for Telehealth in 2026
The 2026 CMS Physician Fee Schedule introduced new Evaluation and Management (E/M) codes to better capture the complexity of telehealth visits.
These updates distinguish between synchronous audio-video and audio-only encounters, reflecting the growing demand for precise coding and accurate reimbursement for virtual care.
1. Synchronous Audio-Video Encounters
These new codes replace traditional in-person E/M visit codes for virtual encounters conducted through real-time audio and video.
Each code corresponds to the time spent and medical decision-making (MDM) complexity.
2. Synchronous Audio-Only Encounters
For telephone visits, audio-only codes have been introduced, but most are not reimbursable under Medicare.
Important:
Only CPT® 98016 is recognized by Medicare as a billable virtual check-in, replacing HCPCS G2012.
Commercial payers may adopt some of the new codes; coders should verify coverage policies specific to each payer.
Also Read: Coding for Telehealth and Telemedicine Services
How These Updates Affect Coding Operations and Compliance
The 2026 telehealth updates are more than administrative adjustments; they reshape how coding teams handle virtual care encounters. Without clear workflows, organizations risk claim rejections, compliance penalties, and longer revenue cycles.

Alt text:How These Updates Affect Coding Operations and Compliance
1. Coding Workflow Adjustments
Coders must review CPT® deletions (99441–99443) and ensure they are removed from templates before January 1, 2025.
EHR systems and billing software should be configured to include the new 98000–98015 codes, even if not all are Medicare-recognized.
Hospitals and billing companies must also map payer-specific coverage rules, especially for commercial and Medicaid plans, which may recognize additional telehealth codes.
Platforms like RapidCode can automatically flag deprecated CPT® codes, map payer eligibility, and update code sets across all specialties.
This ensures compliance on day one of policy rollout, without downtime or manual auditing.
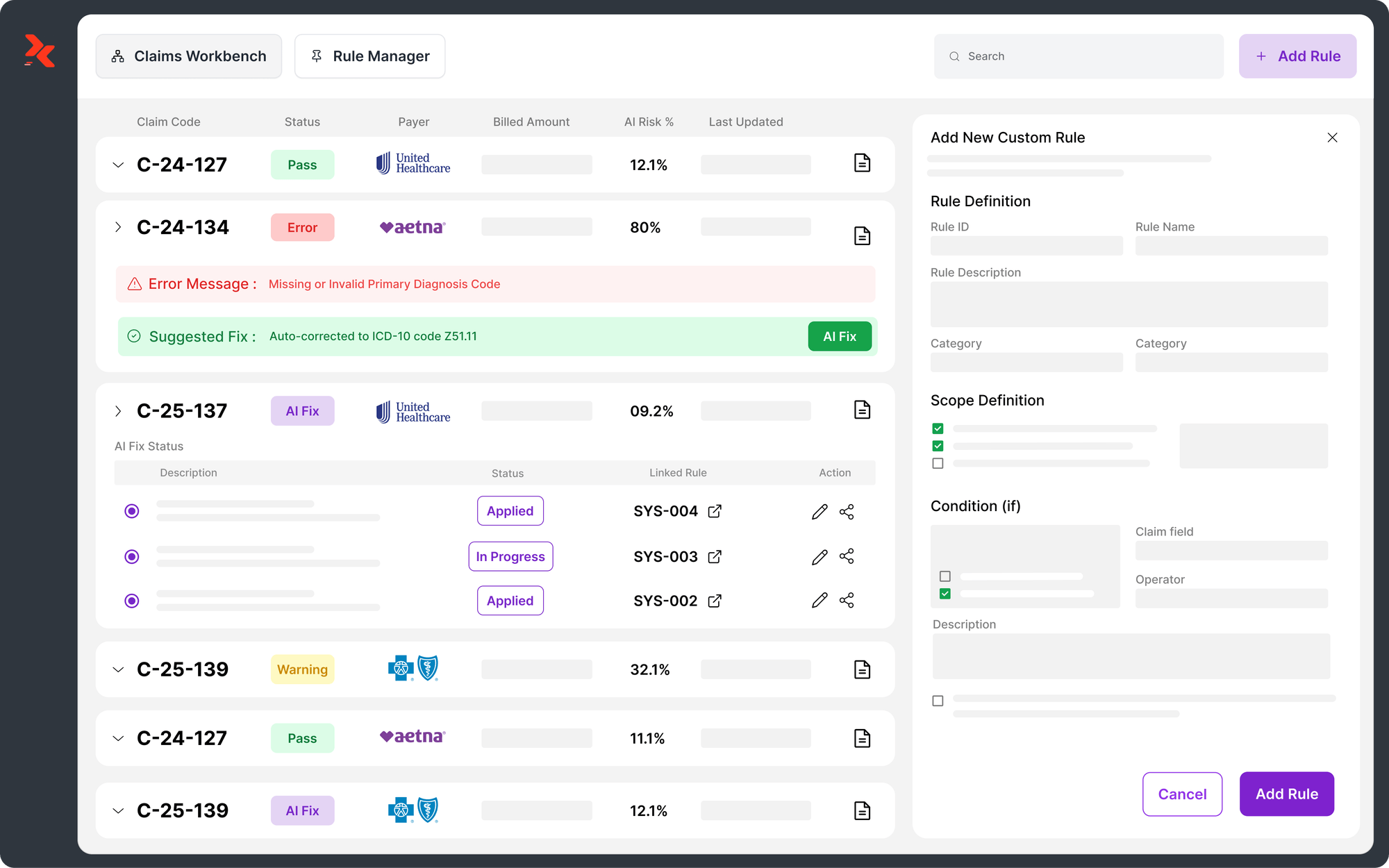
2. Reimbursement and Denial Management
Because Medicare will not recognize most new codes, incorrect submissions could trigger automatic denials.
RCM leaders should:
- Validate payers’ acceptance of telehealth CPT® codes before claims submission.
- Adjust denial prevention rules in their scrubbers to reflect new code statuses.
- Update A/R tracking dashboards for anticipated payment shifts.
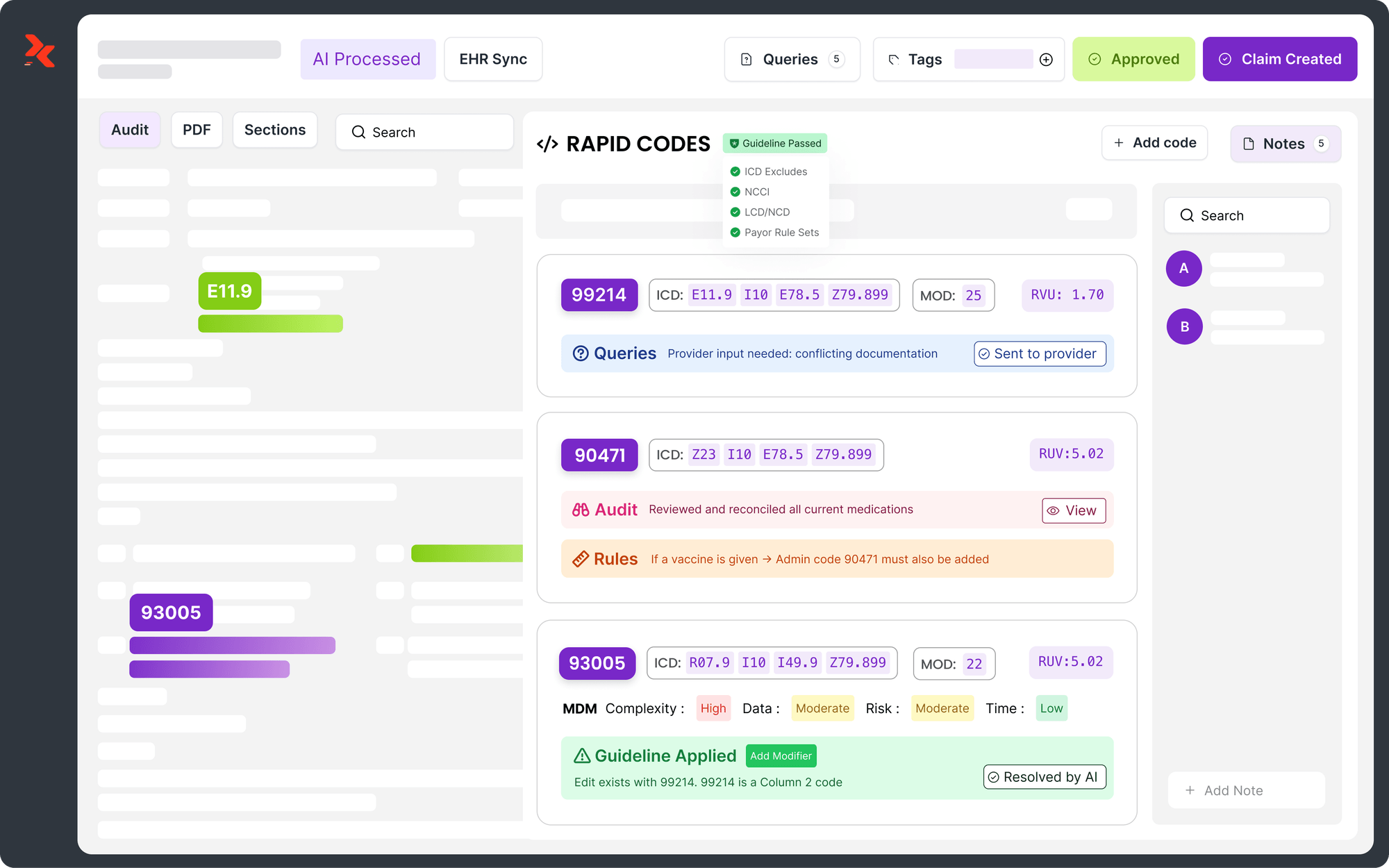
3. Documentation and Audit Readiness
Coders must ensure that time, MDM complexity, and mode of communication (audio vs. video) are clearly documented in encounter notes.
Each telehealth claim should leave an audit-ready trail — a core compliance requirement under ICD-10, CPT®, and CMS guidelines.
Pro Tip:
RapidClaims’ explainable AI models maintain a full audit trail, recording how each CPT® was assigned and which policy rule applied, critical for audit defense and payer review.
Legislative Outlook: Will Congress Intervene?
As of October 2025, the Telehealth Modernization Act of 2024 remains under Congressional review.
If passed, it could permanently remove geographic and site restrictions for Medicare telehealth coverage.
Without action, however, Medicare will revert to pre-pandemic rules, covering only patients in rural or HPSA-designated areas.
This creates an uncertain policy window for providers — especially large physician groups that scaled telehealth beyond rural populations.
Industry associations, including AMA and MGMA, continue to advocate for permanent nationwide coverage.
“The risk of sudden coverage rollback is real,” notes a recent MGMA policy brief. “Providers should prepare contingency workflows, ensuring in-person coverage alternatives if reimbursement restrictions tighten.”
(Source: MGMA, 2025 Telehealth Policy Update)
Preparing for 2026: Key Steps for Providers and Coding Teams
A proactive strategy will help healthcare organizations avoid disruptions when the new telehealth policies take effect.
Telehealth Readiness Checklist
RapidClaims Tip:
RapidScrub automatically integrates updated payer edits, NCCI rules, and CMS bulletins into claim validation, reducing denial probability by up to 70% during policy transitions.
Final Thoughts
The 2026 telehealth updates redefine how providers, coders, and compliance teams operate.
As Medicare narrows telehealth eligibility but expands behavioral health access, the key to maintaining financial stability lies in accurate, adaptive, and compliant coding.
Healthcare organizations should:
- Audit current telehealth claim templates
- Update code sets before January 2026
- Deploy AI-enabled tools to monitor compliance dynamically
RapidClaims empowers healthcare teams to stay audit-ready and revenue-secure by automating policy adaptation, code updates, and payer validation.
Learn more about how RapidClaims AI-driven coding automation keeps your RCM operations future-proof. Request a Demo Now!
FAQs
1. Will Medicare still pay for audio-only telehealth in 2026?
Only in limited cases. CPT® 98016 replaces HCPCS G2012 for brief virtual check-ins. Other audio-only codes (98008–98015) are not recognized by Medicare but may be covered by commercial payers.
2. Are telehealth visits for mental health still covered?
Yes. Behavioral and mental health telehealth services remain permanently covered under Medicare, including therapy and psychiatric evaluations.
3. Which POS codes should be used for telehealth claims?
Use POS 10 when the patient is at home and POS 02 when the patient is in another location. Incorrect POS codes may result in underpayment or claim denial.
4. Do teaching physicians still qualify for virtual supervision?
Yes. Teaching physicians can continue participating virtually for Medicare-covered telehealth through December 31, 2025.
5. How can AI help maintain compliance during this transition?
AI-based coding platforms like RapidClaims automatically synchronize CPT® changes, apply payer-specific rules, and create audit-ready documentation, minimizing human error and policy lag.
.png)
Mary Degapogu
Mary Degapogu is a proficient medical coder with 6 years of experience in E/M Outpatient and ED Profee coding, focused on precise code assignment and documentation compliance to drive clean claims and revenue integrity at RapidClaims.
Latest Post
expert insights with our carefully curated weekly updates
Related Post


.jpg)
Top Products