.jpg)

In urology, billing errors are not minor administrative issues; they directly impact revenue stability, compliance standing, and cash flow performance. Across healthcare, initial claim denial rates have climbed, with recent industry data showing that nearly 12% of all medical claims were denied on first submission in 2024, a continuing upward trend that strains revenue cycle teams and increases operational burden.
Urology’s high procedural volume, complex surgical interventions, frequent modifier application, and evolving payer rules leave little room for inaccuracy. When documentation is incomplete or coding lacks proper alignment, denials rise, payments are delayed, and audit risk increases.
Urology medical billing requires more than basic claim submission. It demands structured documentation, precise CPT and ICD-10 coordination, and consistent oversight throughout the revenue cycle.
This blog examines the operational challenges unique to urology billing and outlines practical strategies to strengthen coding accuracy, reduce denials, and safeguard reimbursement.
At a Glance
- Urology medical billing is high-risk and high-detail. Frequent procedures, modifier use, supply billing, and evolving CPT/HCPCS rules leave little room for error.
- Most denials stem from documentation gaps and modifier misuse. Weak diagnosis linkage, bundling conflicts, and incomplete operative notes are common triggers.
- Clean claim performance requires a structured workflow. Strong documentation, coder validation, pre-submission scrubbing, and ongoing denial monitoring reduce rework and delays.
- AI-driven validation improves accuracy without replacing coders. Automated code suggestions, rule checks, and audit logs help strengthen compliance and increase first-pass acceptance rates.
Table of Contents
- What Is Urology Medical Billing and Coding?
- Why Urology Billing Is More Complex Than Other Specialties
- Core Coding Components in Urology Medical Billing
- Common Urology Coding Mistakes That Lead to Claim Denials
- How to Improve Clean Claim Rates in Urology Medical Billing
- Step-by-Step Workflow: From Clinical Documentation to Clean Claim
- Using AI to Improve Accuracy in Urology Medical Billing
- Real-World Impact: Reducing Denials and Improving Revenue
- Compliance, Audit Readiness, and Risk Management in Urology Billing
- RapidClaims: AI Support for Accurate Urology Medical Billing
- Final Thoughts
- FAQs
What Is Urology Medical Billing and Coding?
Urology medical billing translates clinical services, procedures, and diagnoses into standardized CPT, HCPCS, and ICD-10 codes for reimbursement. The workflow includes patient registration and eligibility verification, detailed clinical documentation, accurate code assignment, claim submission, denial follow-up, and payment reconciliation.
Each stage must align with payer policies to achieve clean claim submission and timely reimbursement.
While the structure of the billing process resembles other specialties, urology adds procedural complexity, frequent modifier use, and strict documentation requirements that increase both financial and compliance risk.
Why Urology Medical Billing Is More Complex Than Other Specialties
Urology spans routine office visits, diagnostic testing, minimally invasive procedures, ambulatory surgery center cases, and complex inpatient operations. Each encounter requires precise coordination of CPT procedure codes, HCPCS supply codes, ICD-10 diagnosis specificity, modifier usage, and compliance with NCCI bundling edits.
Even minor documentation gaps—such as missing laterality, unsupported modifiers, or unclear medical necessity—can result in denials, downcoding, or post-payment review. Ongoing CPT revisions and evolving payer policies add further pressure, particularly for practices operating across clinics, ASCs, and hospitals with different reimbursement methodologies.
In this environment, coding precision directly influences reimbursement performance.
Key Challenges in Urology Coding and Reimbursement
Several recurring issues affect claim accuracy and payment consistency:
- Annual Code Updates: CPT and HCPCS codes are revised each year. Using retired or incorrect codes leads to immediate rejection.
- Modifier and Bundling Errors: Improper application of modifiers such as 25 or 59, and failure to account for NCCI edits, frequently triggers denials.
- Diagnosis-to-Procedure Mismatch: ICD-10 codes must clearly establish medical necessity. Incorrect linkage can invalidate an otherwise accurate CPT code.
- Supply Documentation Sensitivity: Catheter and device billing requires detailed justification of type, frequency, and quantity. Missing documentation often results in claim rejection or audit review.
- Setting-Based Variability: Inpatient encounters affect DRG assignment, while outpatient claims require precise medical necessity alignment. Workflows must adapt to these differences.
Recognizing these pressure points is essential. Addressing them requires disciplined control over the core coding elements that determine claim accuracy.
Core Coding Components in Urology Medical Billing
Strong urology medical billing depends on consistent alignment across four areas: CPT procedures, HCPCS supplies, ICD-10 diagnoses, and modifier usage. Each must be supported by complete documentation to ensure accurate reimbursement and prevent denials.
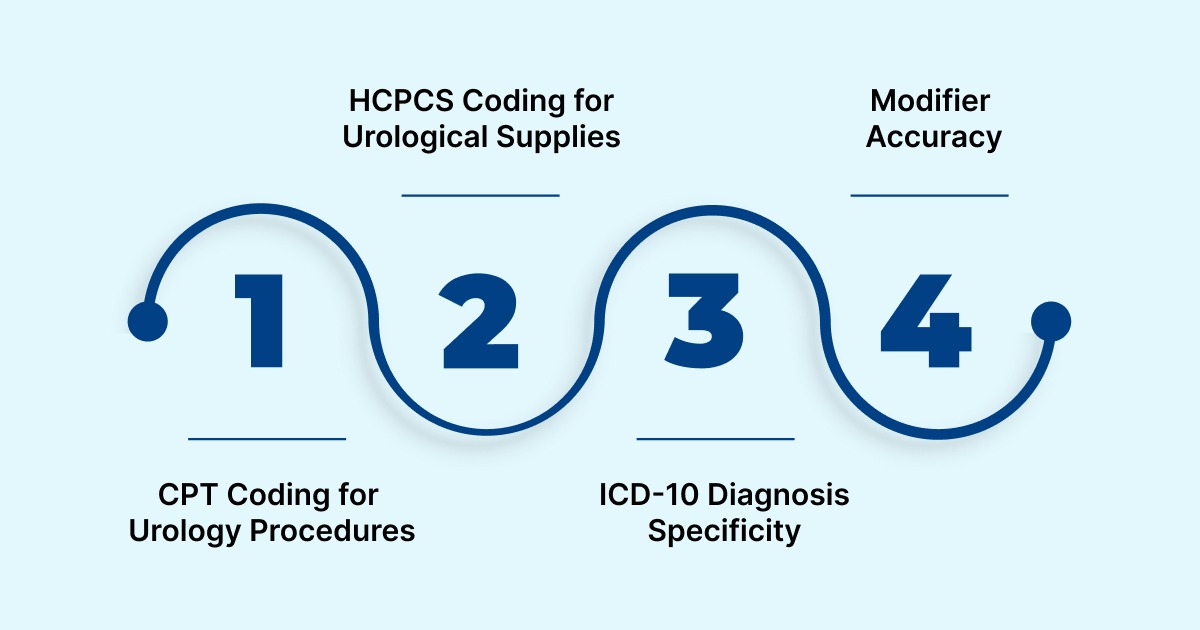
1. CPT Coding for Urology Procedures
Urology includes a broad range of diagnostic and surgical services. Commonly reported CPT codes include:
- 52000 – Cystourethroscopy
- 52310 – Cystourethroscopy with stent removal
- 52281 – Cystoscopy with biopsy
- 52332 – Ureteral stent insertion
- 50590 – Lithotripsy
Operative documentation must clearly reflect clinical indication, technique, laterality, and findings. Coders must verify that services comply with NCCI bundling edits and confirm whether additional procedures are separately reportable.
2. HCPCS Coding for Urological Supplies
Catheters and related devices are billed under HCPCS and are subject to strict coverage limitations. Accurate supply billing requires:
- Clear medical necessity
- Justified quantity and frequency
- Compliance with payer-specific limits
Recent hydrophilic catheter updates, including codes A4295, A4296, and A4297, highlight the need to monitor code revisions and payer policy changes. Unsupported quantities or improper combinations commonly trigger denials.
3. ICD-10 Diagnosis Specificity
Procedural codes must be supported by precise ICD-10 diagnoses that establish medical necessity. Documentation should capture:
- Laterality
- Severity
- Acute versus chronic status
- Complications and related conditions
For example, benign prostatic hyperplasia with lower urinary tract symptoms must be coded with appropriate specificity rather than a generalized prostate diagnosis. Incomplete diagnosis linkage can invalidate otherwise accurate procedure coding.
4. Modifier Accuracy
Modifiers clarify distinct services or clinical circumstances and are frequently required in urology. Common examples include:
- 25 – Separately identifiable E/M service
- 59 – Distinct procedural service
- RT/LT – Laterality
- 26 – Professional component
Each modifier must be supported by documentation that clearly justifies its use. Improper application remains one of the most frequent causes of claim rejection.
When these coding components are consistently aligned with detailed clinical documentation, practices improve clean claim performance and reduce compliance exposure. However, even with a strong understanding of these elements, execution errors still occur.
Common Urology Coding Mistakes That Lead to Claim Denials
Most urology denials are not caused by unfamiliar codes, but by weak documentation, incorrect modifier use, or poor diagnosis linkage. In a specialty where procedures and E/M services often occur together, small inconsistencies can quickly result in rejected claims.
1. Modifier Errors and Bundling Conflicts: Modifiers such as 25, 59 (or XS), RT/LT, and 26/TC must reflect clearly distinct services. If documentation does not support separation—or if NCCI bundling edits are overlooked, claims are likely to be denied or downcoded.
2. Incomplete Operative Notes: Procedural documentation should clearly describe:
- Clinical indication and medical necessity
- Anatomical site and laterality
- Technique performed
- Findings and complications
Missing details can invalidate correct CPT selection and increase audit risk.
3. Same-Day E/M and Procedure Issues: When billing an E/M service with a procedure on the same day, documentation must show that the evaluation was separately identifiable and medically necessary. Without that clarity, modifier 25 is often denied.
4. Diagnosis Mismatch: ICD-10 codes must directly justify the service provided. Insufficient specificity, such as unclear hematuria type or incomplete staging details, can result in medical necessity denials even if the CPT code is accurate.
5. Inconsistent Coding Across Care Settings: Coding standards differ between outpatient clinics, ASCs, and inpatient settings. Failure to adjust for DRG assignment rules or outpatient medical necessity requirements increases denial risk.
Identifying mistakes is useful, but sustainable improvement comes from building structured processes that prevent them in the first place.
Also Read: Navigating the 2026 Evaluation and Management (E/M) Coding Guidelines: Key Highlights
How to Improve Clean Claim Rates in Urology Medical Billing
Improving clean claim rates in urology requires disciplined documentation, accurate coding, and consistent oversight. Because services often involve modifiers, bundling edits, and strict medical necessity requirements, precision at each step directly affects reimbursement.
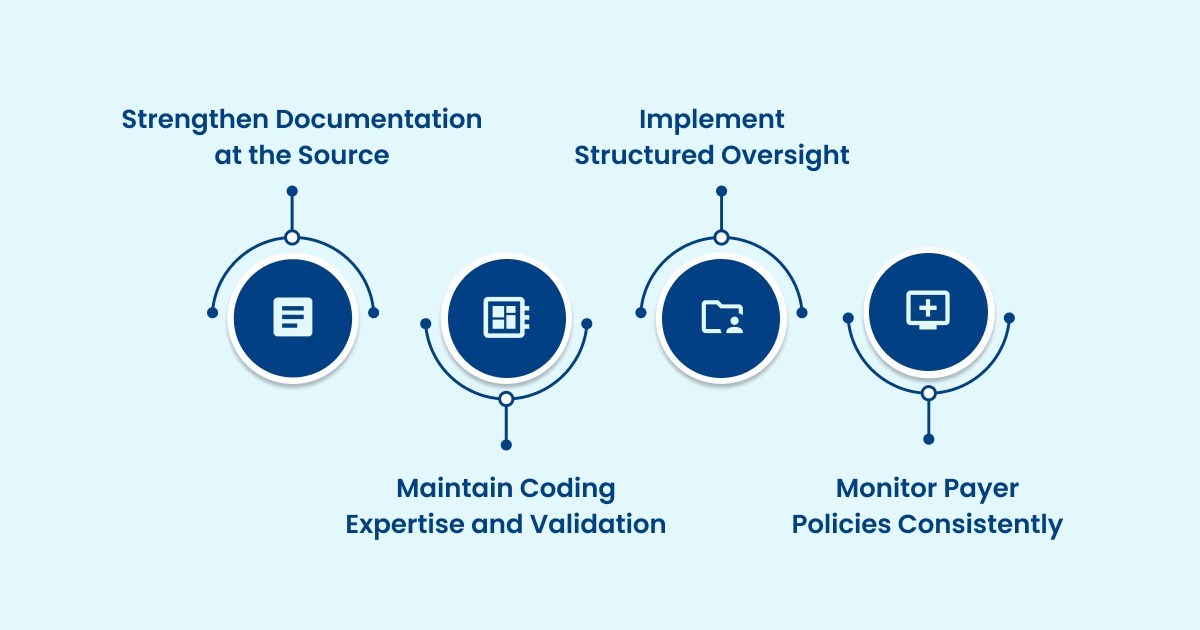
1. Strengthen Documentation at the Source
E/M services must reflect documented medical decision-making complexity or total time, in line with current CMS guidelines. Add-on codes such as G2211 should only be reported when clearly supported.
For procedural services, documentation should clearly include:
- Clinical indication and medical necessity
- Anatomical site and laterality
- Unilateral or bilateral status
- Imaging guidance when applicable
- Complications or additional work performed
ICD-10 diagnoses must also reflect specificity, including severity, chronicity, and related conditions. Incomplete documentation creates ambiguity that leads to denials.
2. Maintain Coding Expertise and Validation
Urology coding requires familiarity with procedural nuances, modifier logic, and payer expectations. Ongoing review of CPT, ICD-10, and payer updates is essential.
While EHR tools may suggest codes, certified coders and providers must validate final selections. Clinical oversight ensures that coding reflects the true scope of care delivered.
3. Implement Structured Oversight
Routine internal audits help detect modifier misuse, bundling conflicts, and diagnosis linkage issues before they become patterns. Reviewing provider coding trends allows early correction and targeted education.
Technology can strengthen this process by validating claims prior to submission and tracking denial trends. However, automation should enhance—not replace—professional review.
4. Monitor Payer Policies Consistently
Coverage rules, prior authorization requirements, and LCD policies vary by payer and change frequently. Practices need a structured process to review updates and confirm that claims align with current contract terms.
Accurate coding supported by complete documentation remains the strongest protection against denials and audit risk.
To make those improvements practical, it helps to view claim accuracy as a defined workflow rather than a series of isolated tasks.
Step-by-Step Workflow: From Clinical Documentation to Clean Claim
Urology encounters often include procedures, devices, imaging, pathology, and follow-up services within the same episode of care. That complexity increases denial risk. Improving clean claim performance requires a defined workflow that begins with documentation and ends with measurable post-submission monitoring.
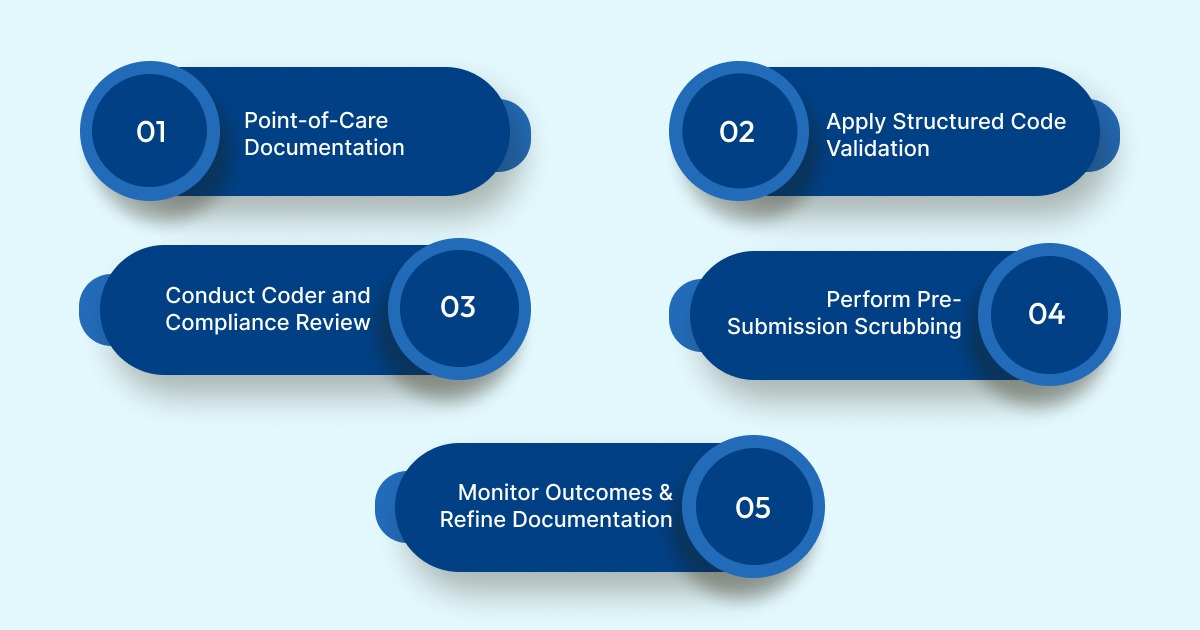
1. Capture Complete Documentation at the Point of Care
Clean claims start with detailed clinical records. EHR templates should prompt providers to document:
- Clear indication and medical necessity
- Relevant history and comorbidities
- Procedural details, including laterality and technique
- Device or catheter type when applicable
- Findings and treatment plan
When imaging or pathology supports the procedure, linking those reports at submission strengthens medical necessity validation and reduces follow-up requests.
2. Apply Structured Code Validation
Coding tools can analyze documentation and suggest CPT and ICD-10 codes while flagging:
- Diagnosis-to-procedure inconsistencies
- Missing documentation elements
- Potential modifier requirements
This reduces manual review time and identifies issues before claims advance in the workflow.
3. Conduct Coder and Compliance Review
Certified coders should confirm:
- CPT and HCPCS accuracy
- ICD-10 specificity and linkage
- Appropriate modifier use, including global period rules
- NCCI edits and MUE limits
- Authorization and payer-specific requirements
High-risk procedures with historical denial trends should receive additional review.
4. Perform Pre-Submission Scrubbing
Before transmission, claims should pass through validation checks to detect:
- Modifier misuse
- Bundling conflicts
- Unit errors
- LCD policy conflicts
- Missing prior authorization
Correcting these issues prior to submission improves first-pass acceptance rates.
5. Monitor Outcomes and Refine Documentation
After submission, teams should track:
- Clean claim rate
- Denial categories and root causes
- Days in accounts receivable
- Payer-specific trends
Successful appeals should inform updates to documentation templates, ensuring that recurring denial patterns are addressed at the source.
Many practices struggle to maintain this level of validation manually. Platforms like RapidClaims embed automated coding review, payer rule validation, and documentation gap detection directly into the workflow, helping teams apply this structure consistently without increasing administrative burden.
As documentation volume increases and payer scrutiny intensifies, relying solely on manual review becomes difficult to sustain. Intelligent validation tools can strengthen this workflow while maintaining clinical oversight.
Using AI to Improve Accuracy in Urology Medical Billing
Urology coding requires interpreting detailed clinical documentation while complying with complex CPT, HCPCS, ICD-10, and payer rules. Manual review alone can slow throughput and still miss subtle errors. AI-driven tools introduce structured validation into the workflow while keeping certified coders in control.
- Automated Code Suggestions: AI uses natural language processing to review operative notes, clinic documentation, and supply records. It identifies key clinical elements and suggests appropriate CPT, HCPCS, and ICD-10 codes. It can also flag required modifiers and missing details such as laterality or procedural specifics. Coders review and confirm these suggestions before submission.
- Pre-Submission Validation: Before a claim is transmitted, AI checks it against payer rules, NCCI edits, MUE limits, and medical necessity standards. It also verifies diagnosis-to-procedure alignment. Catching discrepancies early reduces preventable denials and rework.
- Audit Transparency: AI platforms maintain structured audit logs. These records show how codes were selected and when changes were made. This visibility supports internal compliance review and prepares practices for payer audits.
- Risk Adjustment Support: For Medicare Advantage populations, AI can identify incomplete documentation affecting HCC and RAF scoring. More complete diagnosis capture helps ensure reimbursement reflects patient complexity.
- Practical Integration: AI delivers the most value when embedded into existing EHR and billing systems through API connections or HL7/FHIR integration. A phased rollout, baseline measurement, pilot testing, coder validation, and expansion, helps ensure accuracy and workflow alignment.
When implemented correctly, AI improves coding consistency, strengthens claim validation, and enhances efficiency while preserving clinical judgment.
Also Read: The Role of Artificial Intelligence in Revolutionizing Medical Coding
Real-World Impact: Reducing Denials and Improving Revenue
Structured validation delivers measurable improvements across urology settings.
- Outpatient Clinic: High-volume cystoscopy and biopsy services often generate diagnosis and modifier errors. Automated review flagged missing elements before submission. This reduced manual chart time and improved first-pass acceptance rates.
- Ambulatory Surgery Center: ASCs performing lithotripsy and stent placements frequently encounter HCPCS and bundling denials. Automated cross-checks aligned supply codes with documentation and unit limits. The result was lower claim rework and fewer supply-related rejections.
- Hospital-Based Department: In inpatient settings, improved documentation specificity strengthened DRG alignment. Structured validation reduced audit risk without slowing throughput.
Across all environments, automation shifts coders away from repetitive validation tasks and toward higher-value exception handling. Lower denial rates and faster processing translate directly into stronger financial performance.
Revenue improvement, however, must remain aligned with compliance. Clear documentation, justified modifier use, accurate supply reporting, and consistent policy review ensure that performance gains remain defensible during audits. Validation tools strengthen this discipline, but certified coding oversight remains essential.
As documentation demands and payer scrutiny increase, many urology practices are adopting intelligent validation platforms to reinforce accuracy within existing workflows. One such platform is Rapidclaims.
RapidClaims: AI Support for Accurate Urology Medical Billing
RapidClaims is an AI-powered medical coding and revenue cycle platform designed to improve coding precision and reduce denials without replacing certified coders.
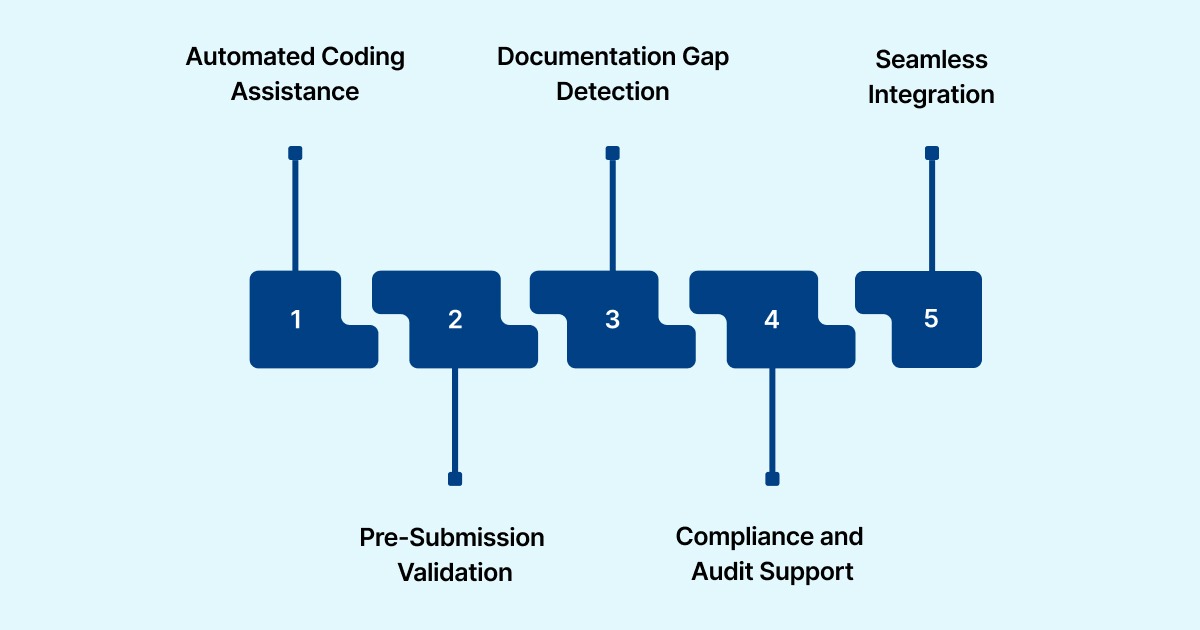
Here are the key features of RapidClaims:
Automated Coding Assistance
- AI-generated CPT, HCPCS, and ICD-10 suggestions
- Modifier recommendations with confidence scoring
Pre-Submission Validation
- NCCI and MUE edit checks
- Payer rule validation
- Diagnosis-to-procedure alignment review
Documentation Gap Detection
- Flags missing laterality, medical necessity details, and procedural specifics
Compliance and Audit Support
- Structured audit logs and override tracking
- Risk adjustment support for HCC/RAF documentation
Seamless Integration
- API-based EHR connectivity
- HL7 and FHIR interoperability
- Real-time and batch processing options
By embedding validation directly into existing workflows, RapidClaims helps urology practices improve first-pass acceptance rates, reduce rework, and maintain regulatory compliance while preserving clinical oversight.
Final Thoughts
Urology medical billing demands precision. Complex procedures, frequent modifier use, and strict payer rules mean small errors quickly turn into denials and revenue delays.
Sustainable improvement comes from structured documentation, accurate code alignment, and proactive claim validation. When review processes and real-time checks are built into the workflow, clean claim rates improve and compliance risk declines.
To see how automated coding validation can strengthen your urology revenue cycle, book a demo with RapidClaims and evaluate the impact firsthand.
Frequently Asked Questions
1. What are the most common errors in urology medical billing?
Frequent errors include modifier misuse, diagnosis-to-procedure mismatches, outdated CPT/HCPCS codes, insufficient supply documentation, and exceeding MUE limits. These issues often lead to denials or downcoding.
2. When should modifier 59 be used in urology coding?
Modifier 59 applies only when procedures are distinct and separately identifiable. Documentation must clearly justify why services are not bundled under NCCI rules.
3. Why is modifier 25 often denied in urology?
Denials occur when documentation does not demonstrate that the E/M service was separate from the procedure performed on the same day. Clear clinical differentiation is required.
4. How do recent HCPCS changes affect urology supplies?
Updated HCPCS codes, including A4295, A4296, and A4297, replaced older catheter codes beginning in 2026. Claims must reflect current codes and include documentation supporting supply type, quantity, and frequency.
5. Why is documentation critical for urological supplies?
Payers require clear evidence of medical necessity, usage frequency, and duration. Missing details frequently result in denials or post-payment audits.
6. How does HCC coding impact urology reimbursement?
Conditions such as prostate cancer and chronic kidney disease can affect Medicare Advantage risk adjustment. Accurate documentation supports proper RAF scoring and reimbursement alignment.


