

Adoption of electronic health record systems has accelerated across the U.S. healthcare system. By 2023, 96% of non-federal acute care hospitals and the majority of office-based physicians were using a certified EHR system. On the surface, adoption looks complete.
Operational reality tells a different story. Many organizations struggle after go-live, as EMRs that were meant to standardize data and strengthen compliance instead introduce friction across clinical, coding, and revenue cycle workflows. Incomplete documentation, coding errors, rising claim denials, delayed reimbursement, and growing audit exposure often follow.
These issues are not caused by the EMR itself. They stem from how systems are implemented, integrated, and governed. Left unaddressed, these gaps quietly erode revenue performance and compliance over time.
This article explores the challenges of electronic medical records and outlines practical ways healthcare leaders can correct them before the impact compounds.
At a Glance
- EMR adoption is high, but performance gaps remain. Poor implementation and weak integration create documentation, coding, and revenue cycle issues after go-live.
- EMR challenges directly impact reimbursement. Interoperability gaps and documentation quality issues lead to coding errors, claim denials, and delayed payments.
- Success depends on operations. Strong governance, clear success metrics, and workflow alignment are critical to EMR effectiveness.
- AI helps stabilize performance post–go-live. Automated documentation review and claim validation reduce rework and denial risk.
- RapidClaims strengthens EMR outcomes. AI-driven coding, documentation support, and pre-submission checks help protect revenue and maintain audit readiness.
Table of Contents
- What Are Electronic Medical Records (EMRs)?
- Why EMR Implementations Fail in Healthcare Organizations
- Major Challenges of Electronic Medical Records in Healthcare
- How EMR Challenges Impact Medical Coding and Claim Denials
- Benefits of Electronic Medical Records When Implemented Correctly
- EMR Use Cases Across Hospitals, Physician Groups, and Billing Companies
- How to Prepare for a Successful EMR Implementation
- Using AI to Address EMR Documentation and Coding Gaps
- How RapidClaims Strengthens EMR Performance After Go-Live
- Conclusion
- FAQs
What Are Electronic Medical Records (EMRs)?
Electronic Medical Records (EMRs) are digital versions of patient charts used within a healthcare organization. They capture clinical data generated during patient encounters, including diagnoses, procedures, medications, lab results, and provider notes.
EMRs replace paper records with centralized, searchable systems that support clinical documentation and internal workflows. While they improve accessibility and consistency of patient information, their real value depends on documentation quality, system integration, and alignment with coding, billing, and compliance processes. Digitizing records alone does not guarantee better operations or outcomes.
Why EMR Implementations Fail in Healthcare Organizations
EMR initiatives are often launched with clear goals, including better documentation, improved care coordination, and more efficient billing. Many fall short not because of system limitations, but because implementation is treated as a technical rollout rather than an operational change.
An EMR affects multiple functions across a healthcare organization, including clinical documentation, coding, billing, compliance, and reporting. When implementation decisions are made in silos, workflows break downstream. Systems often go live without sufficient workflow validation, data quality checks, or reliable integration with coding and billing platforms.
As a result, organizations digitize records without improving documentation quality. Clinical notes may support care delivery but lack the specificity required for accurate ICD-10, CPT, or HCC coding. Coding teams receive incomplete charts, billing teams face higher rejection rates, and compliance teams encounter audit gaps that are difficult to trace.
These gaps directly impact revenue performance, leading to increased rework, inconsistent risk score capture, longer accounts receivable cycles, and higher claim denial rates. Without aligning EMR deployment to data quality, workflow design, and claim outcomes, organizations inherit inefficiencies that persist long after go-live.
These implementation failures are not isolated incidents. They stem from a set of recurring challenges that appear across care settings and system types.
7 Major Challenges of Electronic Medical Records in Healthcare
Electronic Health Records are central to modern healthcare operations. While they improve documentation, reporting, and care coordination, they also introduce structural challenges that affect data quality, compliance, and revenue performance when not managed deliberately.
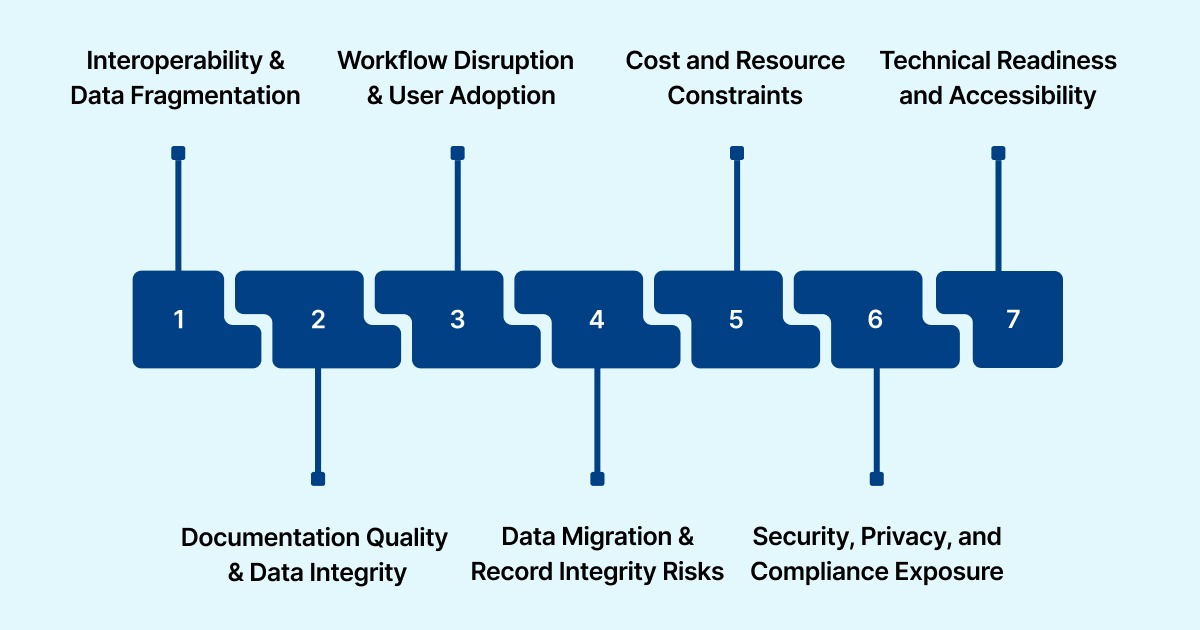
Below are the most common challenges organizations face when implementing and operating EHR systems.
1. Interoperability and Data Fragmentation
EHRs must exchange data with labs, imaging systems, billing platforms, clearinghouses, payer portals, and analytics tools. When integrations are incomplete or inconsistent, data becomes fragmented.
Common issues include:
- Missing diagnosis context across encounters
- Incomplete or outdated problem lists
- Delayed documentation updates between systems
- Manual data re-entry across workflows
These gaps directly affect coding accuracy, claim validation, and revenue cycle efficiency.
2. Documentation Quality and Data Integrity
EHRs are designed for speed, but speed often comes at the cost of clarity. Overuse of templates, copy-forward practices, and disconnected specialty notes reduces clinical specificity.
Typical documentation risks include:
- Insufficient detail to support ICD-10, CPT, or HCC coding
- Propagation of outdated or inaccurate diagnoses
- Inconsistent documentation across visits and providers
Over time, these issues weaken audit defensibility, increase rework, and contribute to higher denial rates.
3. Workflow Disruption and User Adoption
EHR adoption frequently changes how clinicians document care and how administrative teams interpret records. Poor workflow design increases documentation time and introduces workarounds.
Common signs of workflow misalignment:
- Excessive clicks and non-intuitive interfaces
- Inconsistent use of structured fields
- Increased reliance on free-text notes
Resistance is usually operational, not cultural. Systems that slow clinicians down degrade data quality and create downstream inefficiencies.
4. Data Migration and Record Integrity Risks
Legacy data migration is one of the most underestimated aspects of EHR implementation. Errors introduced during migration persist long after go-live.
Frequent migration issues include:
- Duplicate or conflicting patient records
- Incomplete historical documentation
- Incorrect diagnosis or procedure mappings
- Lost audit trails needed for appeals
Poor migration quality introduces long-term coding, billing, and compliance risk.
5. Cost and Resource Constraints
While licensing and infrastructure costs are planned, indirect expenses are often overlooked.
Commonly underestimated costs include:
- Training time and productivity loss during early adoption
- Extended parallel system operations
- Data cleanup and manual rework
- Increased denial management workload
Without success metrics tied to documentation and revenue outcomes, organizations struggle to measure return on EMR investment.
6. Security, Privacy, and Compliance Exposure
EHRs store highly sensitive clinical and financial data and must meet strict regulatory requirements.
Key risk areas include:
- Weak role-based access controls
- Limited visibility into record edits and data lineage
- Gaps in audit logging tied to coding and billing changes
Security failures do not remain isolated to IT. They surface during payer audits, regulatory reviews, and reimbursement disputes.
7. Technical Readiness and Accessibility
EHR performance depends on infrastructure readiness. Aging hardware, limited network capacity, and geographic constraints, especially in rural or underserved settings, affect system reliability.
Without adequate technical capacity and trained staff:
- System access becomes inconsistent
- Documentation quality declines
- Operational effectiveness suffers
EHR challenges are rarely isolated. Interoperability gaps lead to documentation issues. Documentation issues reduce coding accuracy. Coding gaps increase denials and rework. What begins as an EHR limitation ultimately becomes a revenue cycle and compliance problem.
Organizations that invest in governance, workflow alignment, and data quality controls are better positioned to manage these challenges and realize long-term value.
How EMR Challenges Impact Medical Coding and Claim Denials
EMR-related gaps surface most clearly in coding and claims, where documentation quality directly determines reimbursement and compliance outcomes.
a) Documentation Gaps That Affect Coding
Accurate coding depends on complete, specific clinical documentation. Common EMR-driven gaps include:
- Missing or outdated chronic condition status
- Incomplete encounter context for E&M coding
- Weak linkage between diagnoses, assessments, and plans of care
When these elements are absent or unclear, coders are forced to interpret intent, increasing the risk of undercoding, overcoding, or claim rejection.
b) Increased Claim Denials and Rework
Claims that lack adequate documentation support are flagged by payer edits or denied outright. Even when care delivery is appropriate, insufficient documentation triggers rework, raises operational costs, and delays reimbursement.
c) Risk Adjustment and HCC Impact
For Medicare Advantage and value-based care programs, EMR documentation quality directly affects HCC capture. Inconsistent problem lists, missing condition updates, or undocumented diagnoses lower RAF scores and misrepresent population risk, reducing reimbursement across the contract year.
These impacts are not inevitable. When EMR implementation aligns documentation practices with coding and revenue workflows, organizations can improve accuracy, reduce denials, and stabilize reimbursement outcomes.
Benefits of Electronic Medical Records When Implemented Correctly
When electronic medical records are implemented with clear governance and workflow alignment, they deliver measurable operational and clinical benefits rather than just digital storage.

- Faster Access to Accurate Information: EMRs give clinicians, coders, and billing teams immediate access to current patient data, including diagnoses, medications, and encounter history. Real-time availability reduces delays caused by manual record retrieval and improves coordination between clinical and administrative teams, particularly during handoffs and urgent care scenarios.
- Lower Administrative Overhead: By eliminating paper storage, printing, and manual record handling, EMRs reduce ongoing administrative costs. Standardized digital workflows also shorten the time spent on internal record requests, chart reviews, and follow-ups, allowing staff to focus on higher-value tasks.
- More Consistent and Reliable Documentation: Structured documentation within EMRs improves consistency across providers and departments. This reduces errors caused by illegible or incomplete notes and supports clearer clinical narratives, which are essential for accurate coding, audit readiness, and continuity of care.
How these benefits materialize varies by organization type. Hospitals, physician groups, and billing companies each face different constraints and priorities.
EMR Use Cases Across Hospitals, Physician Groups, and Billing Companies
MRs deliver the most value when aligned to the operational realities of different healthcare organizations. While the underlying technology may be similar, deployment priorities and success criteria vary by care model.
i) Hospital Systems
Large hospital systems manage high encounter volumes across multiple specialties, making standardization and governance essential.
Key EMR priorities include:
- Phased rollouts to minimize disruption across departments
- Specialty-specific documentation templates to preserve clinical detail
- Early integration with coding and billing workflows
- Embedded coding validation to reduce departmental variation
When these elements are in place, hospitals see fewer denials, less rework, and more predictable revenue performance.
ii) Multi-Specialty Physician Groups
Physician groups often operate with lean teams and tight margins, placing a premium on efficiency.
Effective EMR use focuses on:
- Documentation workflows aligned to specialty-specific practices
- Minimal clicks and reduced reliance on free-text entries
- Structured templates that support coding requirements
- Pre-submission coding validation without increasing staff
These practices improve first-pass claim acceptance, reduce coder backlogs, and shorten billing cycles.
iii) Medical Billing Organizations
Billing companies depend on consistent data quality across multiple client EMRs.
Successful EMR strategies emphasize:
- Clear integration standards across client systems
- Normalized data structures for scalable processing
- Reliable audit trails to support payer disputes
- EMR-integrated automation to handle volume growth
This approach allows billing organizations to scale operations while maintaining accuracy and control.
Also Read: How Medical Billing and Coding Help Boost Revenue
Across all use cases, EMR success depends less on the platform itself and more on preparation, governance, and disciplined execution.
How to Prepare for a Successful EMR Implementation – Strategies
Overcoming EMR challenges requires an operational approach that goes beyond system configuration. The most effective strategies focus on governance, workflow alignment, and continuous validation across clinical and revenue teams.

Step 1: Establish Governance and Ownership
Start by defining who owns EMR decisions across the organization. EMRs affect clinical documentation, coding, billing, compliance, and IT, so governance must be cross-functional.
Key roles should include:
- Clinical leaders to set documentation standards
- Coding and revenue cycle leaders to ensure downstream accuracy
- IT leaders to manage integrations and system performance
- Compliance leaders to maintain audit readiness
Clear ownership and escalation paths prevent last-minute trade-offs that weaken data quality and workflows.
Step 2: Define Success Metrics Before Go-Live
Adoption alone does not equal success. Before implementation begins, define metrics that reflect operational and revenue outcomes.
Track metrics such as:
- Clean claim rate
- Denial rate by payer and reason
- Coding turnaround time
- Time from encounter to final bill
- Audit exception frequency
These KPIs ensure EMR performance is measured by its impact on documentation, coding, and reimbursement.
Step 3: Validate Workflows and Integrations
Before scaling, test workflows using real clinical and billing scenarios. Validation should confirm that documentation flows correctly from encounter to coding and claims.
Validation should include:
- ICD-10, CPT, and HCC documentation support
- Accurate data transfer to billing systems
- Handling of late documentation and amendments
- Preservation of audit trails
Early validation reduces post–go-live rework and denial risk.
Step 4: Plan Role-Based Training and Change Management
EMRs change how clinicians document and how downstream teams use records. Training must reflect real workflows, not generic system features.
Preparation should include:
- Role- and specialty-specific training
- Clear documentation expectations
- Early feedback loops to address friction
Without structured change management, documentation quality declines even when systems function as designed.
Step 5: Prepare for Scale and Ongoing Optimization
EMR implementation does not end at go-live. Organizations must plan for growth, regulatory changes, and evolving payer requirements.
Ongoing preparation includes:
- Performance testing during peak volumes
- Defined downtime and recovery procedures
- Regular documentation and coding audits
- Continuous monitoring of denial trends
Even with careful preparation, manual processes alone cannot keep pace with documentation and coding complexity at scale. Automation becomes essential to maintain accuracy, reduce rework, and support consistent revenue performance over time.
Using AI to Address EMR Documentation and Coding Gaps
AI helps close documentation and coding gaps that commonly arise in EMR environments and are difficult to manage through manual review alone. When implemented with proper controls, AI improves data quality and claim outcomes without adding operational complexity.
- Automated Documentation and Coding Review: AI analyzes structured fields and free-text clinical notes to identify missing diagnoses, unsupported procedures, and incomplete documentation before charts are finalized. Early detection reduces follow-up queries, shortens chart completion time, and improves the reliability of coding inputs.
- Pre-Submission Claim Validation: AI-based validation checks EMR data against payer-specific coding and medical necessity rules before claims are submitted. This allows teams to address issues while documentation is still current, increasing first-pass acceptance rates and reducing avoidable denials.
- Governance and Human Oversight: Effective AI use requires clear governance. Human review, confidence thresholds, and audit controls ensure outputs remain explainable, compliant, and aligned with organizational standards. These safeguards enable automation at scale while maintaining accountability across coding and billing workflows.
As organizations move beyond basic EMR adoption, automation becomes essential to closing operational gaps. Platforms that connect documentation quality, coding accuracy, and revenue outcomes help teams use EMR data productively rather than letting it slow workflows down.
One such platform is RapidClaims, an AI-driven solution built specifically for revenue cycle operations. RapidClaims embeds automation directly into existing workflows to reduce manual effort, surface issues early, and stabilize performance after EMR implementation.
How RapidClaims Strengthens EMR Performance After Go-Live
RapidClaims supports clinical and revenue teams through:
- RapidCode – Autonomous medical coding for ICD-10, CPT, and E&M services, reducing manual workload and improving consistency
- RapidScrub – Pre-submission claim validation that identifies and resolves issues before payer review
- RapidCDI – Documentation support that improves diagnosis specificity and risk adjustment accuracy
- Seamless integration – Works with major EHR and billing systems without disrupting existing workflows
- Governed AI – Transparent outputs and audit trails that support compliance and oversight
Together, these capabilities help organizations reduce denials, accelerate reimbursement, and protect revenue as documentation patterns evolve. RapidClaims complements EMR investments by ensuring data quality and revenue performance remain stable well beyond go-live.
Learn how to overcome challenges of electronic medical records, improve documentation quality, reduce denials, and protect revenue performance.
Conclusion
The above challenges of electronic medical records extend well beyond go-live. When documentation gaps, workflow misalignment, and weak validation persist, they directly impact coding accuracy, claim acceptance, and reimbursement timelines.
Organizations that treat EMRs as operational infrastructure, not one-time IT deployments, see stronger results. Ongoing governance, measurable performance tracking, and continuous validation help ensure documentation quality and revenue performance remain stable over time.
AI-driven platforms like RapidClaims support this approach by validating documentation and coding as workflows evolve, helping organizations reduce denials and maintain audit readiness after implementation.
Book a demo to explore AI-driven coding, documentation validation, and claim checks in action.
FAQs
1. What are the biggest challenges of electronic medical records?
Interoperability gaps, workflow misalignment, data migration errors, documentation quality issues, and downstream impacts on coding and revenue cycles are the most common challenges.
2. Why do EMR implementations often increase claim denials initially?
Early post–go-live periods typically surface documentation gaps, workflow disruptions, and inconsistent data entry, which trigger coding errors and payer edits until processes stabilize.
3. How long does EMR implementation usually take?
Most implementations take 6–12 months, depending on organizational size, integration complexity, and whether the rollout is phased or organization-wide.
4. How does EMR data quality affect coding and claims?
Incomplete or inconsistent documentation leads to inaccurate ICD-10, CPT, or HCC coding, resulting in medical necessity denials, rework, and delayed reimbursement.
5. Do EMRs support accurate HCC risk adjustment by default?
Not necessarily. Risk adjustment accuracy depends on consistent condition documentation, encounter linkage, and ongoing review across visits.
6. Can AI help reduce EMR-related denials and compliance risk?
Yes. When deployed with audit controls and human oversight, AI can identify documentation gaps, validate coding, and flag claim issues before submission.


